“Medicinal cannabis has gained increasing attention from both the scientific community and clinical practice, due to the therapeutic potential of its major phytocannabinoids, particularly cannabidiol (CBD) and Δ9-tetrahydrocannabinol (THC), for pain management.
This review compiled and analyzed the available evidence regarding the antinociceptive effects of nanoencapsulated cannabinoids compared to free compounds. The published works have explored some pharmaceutical formulations and administration routes on different acute, chronic and neuropathic pain experimental models.
The findings indicated that cannabinoids exhibited promising analgesic effects, while nanoencapsulation could enhance its stability and bioavailability.
Despite these advances, the number of reports investigating nanostructured cannabinoid-based systems remains limited, with a predominance of preclinical research. A recurrent lack of structural information and quality control data for such works was also noted. Furthermore, there were not identified any research regarding the nanoencapsulation of full-spectrum cannabis oils or whole cannabis extracts, highlighting a significant gap in the current literature.
Overall, nanoencapsulation emerges as a versatile strategy to overcome the intrinsic limitations of cannabinoids and expand its clinical applicability for pain treatment. Nevertheless, further efforts are required to determine standardized methodologies, facilitating the translation of preclinical findings into clinical practice, in order to provide stable, safe, effective and more accessible cannabinoid-based therapies.”
“Overall, advances in the nanoencapsulation of cannabinoids and other cannabis-derived products can significantly contribute to the development of stable, safe, effective and cost-effective pain therapies, particularly for chronic and neuropathic pain conditions.”
“Background/Objectives: Current literature regarding the efficacy of cannabis to reduce chronic pain intensity is mixed. Despite growing accessibility throughout the U.S., it is still unclear if the naturalistic use of recreational cannabis edible products is associated with decreases in pain intensity on days of use or longitudinally, and if these associations are dependent on the doses of delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) being consumed.
Methods: The trial (NCT03522324) from which these data were pulled was pre-registered in April 2018. Participants (N = 243; 56% female; mean age = 46 ± 12 years) with self-reported chronic low-back pain selected a recreational edible cannabis product to use exclusively, ad libitum, for 14 days. Labeled THC and CBD potency were used to determine product group: CBD-dominant (n = 97), THC + CBD (n = 112), or THC-dominant (n = 34). Participants completed daily surveys indicating current pain intensity (PROMIS; 0-10 scale), use or non-use of their product, and cannabinoid dose (THC and CBD).
Results: Linear mixed effects showed a significant use × group interaction (p = 0.002), indicating that pain intensity was significantly lower on days of use in THC-dominant (b = -0.66, 95% CI [-0.94,-0.37]) and THC + CBD (b = -0.41, 95% CI [-0.57,-0.25]) groups compared to days when cannabis was not used. A significant group × time interaction (p = 0.02) indicated that pain intensity significantly decreased from day 1 to day 14 in those using THC + CBD products (b = -0.05, 95% CI [-0.07,-0.03]), with 36.6% of participants in the THC + CBD group experiencing ≥30% reduction in pain intensity from day 1 to day 14. Increasing doses of THC (b = -0.02, 95% CI [-0.04, -0.01]), not CBD (b = 0.003, 95% CI [-0.03, 0.01]), were associated with significantly lower pain intensity on days following product use, with increasing doses of CBD diminishing the impact of THC dose (b = 0.02, 95% CI [0.01, 0.04]).
Conclusions: These findings indicate a complex relationship between THC, CBD, and pain intensity associated with the naturalistic use of recreational cannabis edible products. Lower daily pain intensity was associated with the use of products containing THC; however, dose models indicate that this association may be attenuated at higher doses of CBD. Additionally, only products containing relatively equal amounts of THC and CBD were associated with lower pain intensity after 14 days of observation.”
“Daily data collected over 14 days of naturalistic cannabis use demonstrated that reductions in participants’ current pain intensity were associated with the use of cannabis edible products, but only in products that contained THC. More frequent use of these products in the previous 24 h was associated with improved reductions in pain intensity.”
“Background: Fibromyalgia (FM) is a chronic pain condition characterized by widespread pain, fatigue, and functional impairment. Current pharmacological treatments show limited efficacy and poor tolerability. Cannabidiol (CBD) has demonstrated analgesic and anti-inflammatory properties, but evidence regarding CBD-containing topical formulations in FM remains scarce.
Objectives: To evaluate the feasibility, safety, and preliminary efficacy of a CBD-containing topical formulation for localized pain in patients with FM and to explore its potential impact on broader symptom domains.
Material and methods: This single-arm pilot study included 30 women with FM and clinically relevant localized pain due to musculoskeletal, neuropathic, or cutaneous comorbidities. Participants self-applied a commercially available CBD-containing topical formulation to a painful area every 8 h for 12 weeks. Outcomes were assessed at baseline, 4 weeks, and 12 weeks. Nonparametric repeated-measures analyses, Monte Carlo resampling, effect sizes, and minimal clinically important difference (MCID) thresholds were applied.
Results: At the 4- and 12-week follow-up visits, all participants reported full adherence to the prescribed application schedule. No adverse events or side effects were reported. Localized pain showed a significant and clinically meaningful reduction at 4 weeks, sustained at 12 weeks (60% achieving MCID). Functional capacity improved significantly, with 50% of participants exceeding the MCID at 4 weeks. Widespread Pain Index (WPI) and Symptom Severity Scale (SSS) scores decreased progressively, and a lower proportion of participants met the 2010 American College of Rheumatology (ACR) diagnostic criteria for FM at 12 weeks, while generalized pain, fatigue, anxiety, and depression did not show significant changes.
Conclusions: Topical application of a CBD-containing formulation was feasible and was associated with improvements in localized pain and functionality in this exploratory single-arm study. Changes observed in WPI and SSS, and in the proportion of participants meeting the 2010 ACR criteria at follow-up, should be interpreted cautiously and considered exploratory and hypothesis-generating, given the uncontrolled design (precluding causal inference), the symptom-based and fluctuating nature of FM, and the multicomponent composition of the product. Although limited by its uncontrolled design, this pilot study provides effect size estimates and methodological guidance to support future randomized controlled trials of topical cannabinoids in FM.”
Background: Chronic neuropathic pain (NP) is frequently accompanied by anxiety- and depression‑like symptoms, reflecting maladaptive interactions between nociceptive and affective brain networks. The anterior insular cortex (AIC) integrates sensory and emotional dimensions of pain and represents a potential target for pharmacological modulation. Cannabidiol (CBD) exhibits analgesic and anxiolytic/antidepressant‑like properties through interactions with endocannabinoid and serotonergic systems.
Objectives: We investigated whether CBD microinjection into the AIC modulates NP and its affective comorbidities, and whether these effects depend on CB1 and 5‑HT1A receptors.
Methods: Male Wistar rats were subjected to chronic constriction injury (CCI) of the sciatic nerve. Fourteen days later, guide cannulae were implanted into the AIC. On day 21 post‑CCI, animals received intra‑AIC microinjections of CBD (15, 30, or 60 nmol/200 nL) or vehicle. Mechanical (von Frey test) and cold (acetone test) allodynia, anxiety‑like behavior (open field and elevated plus maze tests), and depression‑like behavior (forced swim and sucrose spray tests) were assessed by different psychobiological tests. The role of cannabinoid and serotonergic receptors was addressed by intra‑AIC pretreatment with either the CB1 receptor antagonist AM251 or the 5‑HT1A receptor antagonist WAY-100,635 in independent groups.
Results: AIC pretreatment with CBD dose‑dependently reduced mechanical and cold allodynia and anxiety‑ and depression‑like behaviors, with the most robust effects observed at 60 nmol. AIC Pretreatment with either AM251 or WAY-100,635 abolished the antinociceptive and affective effects of CBD.
Conclusion: CBD administration within the AIC produces integrated analgesic, anxiolytic, and antidepressant-like effects in a model of neuropathic pain. These effects are consistent with the involvement of CB1 and 5-HT1A receptor signaling. The findings identify the AIC as a relevant cortical substrate linking nociceptive and affective processes and support CBD as a promising psychopharmacological strategy for NP associated with emotional comorbidities.”
“In conclusion, this study demonstrates that CBD microinjection into the AIC attenuates mechanical and cold allodynia while also reducing anxiety- and depression-like behaviors in an experimental model of NP.”
“Overall, these findings highlight the AIC as a potential neural substrate involved in the interaction between chronic pain and its emotional comorbidities and identify CBD as a promising psychopharmacological approach for NP conditions associated with affective dysfunction.”
“Background/Objectives: Chronic low back pain (CLBP) affects approximately 20% of the global population and is a leading cause of years lived with disability. Long-term, real-world evidence for inhaled cannabis in patients refractory to conventional multimodal therapy remains scarce. We assessed the five-year efficacy and safety of inhaled cannabis in CLBP patients who had documented failure of ≥1 year of opioid analgesics, anticonvulsants, antidepressants, NSAIDs, and physiotherapy, with each patient serving as their own historical control.
Methods: We analyzed prospectively collected clinical data from 241 consecutive adults with treatment-refractory CLBP (mean age 49.3 ± 14.9 years; 37.8% female; mean pain duration 15.1 years) initiated on inhaled medical cannabis (predominantly smoking, THC 4-22%, CBD 2-22%) in a single-center tertiary orthopedic clinic between 2020 and 2025 (Hasharon Hospital, Rabin Medical Center, Israel; IRB protocols 0807-21-RMC and 0634-25-RMC). Year-0 outcomes during conventional therapy were compared with outcomes at Years 1-5 on cannabis. Primary outcomes were the Numeric Rating Scale (NRS), Oswestry Disability Index (ODI), and Brief Pain Inventory severity/interference (BPI-S/BPI-I). Concomitant-medication trajectories were a secondary outcome. The primary analysis was a mixed model for repeated measures (MMRM) with random intercept and slope, REML estimation, and time as a categorical fixed effect. Multiple imputation (MAR, m = 20, Rubin’s rules) was the primary missing-data approach; complete-case and tipping-point pattern-mixture sensitivity analyses were used. A multivariate Hotelling T2 provided a joint test across the four correlated PROMs. Concomitant-medication discontinuation was modeled with GEE logistic regression and exact McNemar tests. Time to discontinuation was estimated by Kaplan-Meier and Cox regression. The Bonferroni-adjusted significance threshold for the four primary outcomes was α = 0.0125. BioWell gas-discharge-visualization (GDV) parameters were exploratory only.
Results: Of 241 patients, 238 (98.8%) provided Year-5 data and 224 (92.9%) remained on cannabis at Year 5; only five patients (2.1%) discontinued for adverse events or inefficacy. All four primary PROMs improved markedly and durably. MMRM-estimated Year-5 minus Year-0 changes were: NRS -5.36 (95% CI -5.65, -5.07), ODI -17.68 (95% CI -19.73, -15.63), BPI-S -6.73 (95% CI -6.99, -6.47), and BPI-I -3.41 (95% CI -3.65, -3.16); all four contrasts had |z| ≥ 16.9 and p < 10-20. MI-pooled estimates were within 0.05 of MMRM (FMI < 0.03 for all outcomes). Hotelling T2 was F(4, 232) = 872.8, p < 10-20. At Year 5, 89.2% achieved ≥30% NRS reduction, 77.2% ≥ 50%, and 93.4% met the NRS minimum clinically important difference (MCID); ODI MCID 65.6%, BPI-S MCID (≥1 pt) 98.3%, BPI-I MCID (≥1 pt) 91.3%. Concomitant opioid use fell from 100% at baseline to 4.6% at Year 5 (within-patient absolute risk reduction 95.4%, McNemar exact p = 1.16 × 10-69), NSAID from 100% to 7.1%, SSRI/SNRI from 80.5% to 5.4%, and gabapentinoid from 38.6% to 2.5%. The ARR-derived NNT for opioid discontinuation was 1.05; this NNT is referenced to each patient’s own documented maximal-conventional-therapy state and is not equivalent to a between-arm randomized-trial NNT. Cannabis dose × time interaction was consistent with no pharmacological tolerance (β = -0.0044 per gram-month per year, p = 0.074). Across 1205 patient-years of cannabis exposure (calculated as 241 patients × 5 follow-up years from Year 1 through Year 5; baseline Year 0 represents pre-cannabis state and is not included in person-time on cannabis), 1338 organ-system AE events were recorded at 1.110/patient-year (Poisson 95% CI 1.05-1.17); 99.8% of graded events were mild (grade 1), with ocular (476 events, 0.40/PY), cognitive (460, 0.38/PY), and gastrointestinal (368, 0.31/PY) reactions predominating. The Year-3 retention dip reflected a documented telemedicine-clinic phenomenon during 2022-2024, with patients returning to in-person follow-up by Year 4-5. BioWell GDV discriminated NRS ≥ 4 only at chance level (BWS AUC 0.574, 95% CI 0.54-0.60; BWV AUC 0.51).
Conclusions: In a treatment-refractory CLBP cohort with five-year longitudinal follow-up, inhaled cannabis was associated with large, sustained, and statistically robust improvements in pain, disability, and pain interference, accompanied by near-total displacement of opioids, NSAIDs, antidepressants, and gabapentinoids. These observational associations, although mechanically less susceptible to bias for the binary medication-discontinuation outcomes than for self-reported PROMs, cannot be interpreted causally in the absence of a concurrent randomized control arm and may reflect a combination of pharmacological effect, regression to the mean from a high pre-treatment baseline, expectancy and self-selection effects intrinsic to an actively chosen open-label therapy, and secular trends in pain reporting. The within-patient benefit-risk profile-ARR-derived NNT ≈ 1 for opioid sparing against a predominantly mild adverse-event burden-supports consideration of cannabis as a potentially clinically meaningful, opioid-sparing option in patients who have failed multimodal conventional therapy, pending confirmation in randomized comparative trials.”
“Inhaled medical cannabis has emerged as a candidate analgesic for refractory chronic-pain syndromes.
Mechanistically, exogenous Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD) modulate the endocannabinoid system through CB1- and CB2-receptor signaling, with downstream effects on descending pain modulation, peripheral nociceptor sensitization, and affective dimensions of suffering.”
“These data support consideration of inhaled cannabis as a potentially clinically meaningful, opioid-sparing option for patients who have failed conventional multimodal therapy.”
Background: Opioid withdrawal is a significant challenge for people seeking to reduce or eliminate opioid use, and unmanaged withdrawal increases the risk of relapse and overdose. Using cannabis to manage opioid withdrawal has been reported by people who use opioids, yet it is not clear whether this leads to reductions in opioid use. Moreover, because pain is prevalent among people who use unregulated opioids (PWUO) and may contribute to ongoing opioid use, the effects of cannabis use to manage withdrawal symptoms may differ among individuals experiencing moderate to severe pain. We investigated the relationship between cannabis use to manage unregulated opioid withdrawal and self-reported reductions in opioid use among PWUO.
Methods: Data were derived from a cross-sectional questionnaire administered to cannabis-using PWUO in Vancouver, Canada, between December 2019 and November 2021. Multivariable logistic regression estimated the associations between cannabis use for opioid withdrawal and self-reported reductions in opioid use. A sub-analysis explored if these associations varied among participants living with and without moderate to severe pain.
Results: Among 197 participants, 89 (45.2%) reported cannabis use to manage symptoms of opioid withdrawal in the past six months. In multivariable analysis, cannabis use for opioid withdrawal was significantly associated with self-reported reductions in opioid use (adjusted Odds Ratio [AOR] = 2.16, 95% Confidence Interval [CI]: 1.13-4.19) in the same time period. In a sub-analysis, this association was only significant among participants with moderate to severe pain (AOR = 6.55; 95% CI: 2.44-19.63).
Conclusions: We observed a significant association between self-reported use of cannabis to manage unregulated opioid withdrawal and reductions in opioid use among cannabis-using PWUO living with pain. Aligned with other studies, these findings support conducting experimental trials of cannabinoids to support individuals experiencing opioid withdrawal and living with pain.”
“Cannabinoid-based therapies have gained increasing attention for the management of chronic and treatment-resistant pain, although their clinical application is limited by the poor aqueous solubility and variable bioavailability of Δ9-tetrahydrocannabinol (THC).
In this study, we developed and characterized a nanoemulsion (THC-NE) for buccal administration of a Cannabis sativa L. extract (Bedrocan®), with the aim of improving solubility, stability and bioavailability.
The optimized formulation, composed of pharmaceutically acceptable excipients, showed a narrow droplet size distribution (DH ≈ 73 nm, PDI ≈ 0.2), a THC content consistent with the theoretical value (3.53 ± 0.56 mg/mL), and good physicochemical stability at 4°C for at least 90 days. The formulation maintained its properties upon extensive dilution in simulated buccal fluids and after spray nebulization, supporting its suitability for oromucosal delivery. In vitro release studies confirmed sustained THC release from THC-NE, whereas negligible release was observed from the oil extract, highlighting the role of nanoformulation in enhancing solubilization and controlled release.
An observational study was conducted in 18 patients with chronic pain unresponsive to standard treatments. After a median follow-up of 189 days, mean pain scores (NRS) decreased significantly from 8.6 ± 0.9 to 5.4 ± 2.8 (p < 0.001), with 83% of patients achieving a ≥ 20% reduction. Among responders, the mean NRS decreased by 45% and treatment persistence was found to be high, with 64% of patients still remaining under therapy after six months. A total of 17 adverse events were reported in 11 patients, most of which were mild to moderate and transient. Additionally, treatment interruption occurred in three patients due to adverse events, in other three owing to limited efficacy and in two for logistical reasons.
Overall, these findings indicate that buccal administration of THC-NE represents a promising patient-friendly approach for cannabis-based therapy, offering improved solubility, controlled release and meaningful clinical benefit in patients with refractory chronic pain.”
“Among the bioactive compounds found in Cannabis sativa, Δ9-tetrahydrocannabinol (THC) has been identified as the primary psychoactive component, exhibiting significant analgesic, antispastic, and neuroprotective properties. “
“This study demonstrates that NE technology can be successfully applied to develop a stable and efficient buccal formulation of Cannabis sativa extract. The optimized THC-NE proved to be physicochemically stable, robust under dilution, and suitable for administration via standard spray devices, while ensuring enhanced release of THC compared to the oily extract.”
“Cannabinoid-based therapies have shown analgesic, anti-inflammatory, and wound-healing potential across veterinary species; however, clinical data on long-term use of THC-rich formulations in horses remain scarce.
This case report describes the use of combined oral and topical THC-rich and CBD-rich full-spectrum cannabis oils as part of a palliative care strategy in a rescued horse with severe chronic disease.
A senior mixed-breed gelding was rescued with a large, chronic ulcerative lesion of the left hind limb, severe malnutrition, non-weight-bearing lameness (AAEP grade 5/5), and refractory pain. Diagnostic workup identified a fibroblastic equine sarcoid complicated by complete suspensory tendon rupture, early osteomyelitis, and chronic joint disease. Conventional medical and surgical options were limited due to poor response, disease severity, and resource constraints.
A long-term palliative protocol was initiated using oral THC-rich and CBD-rich full-spectrum cannabis oils (1:1 ratio; 100 mg/mL each) with gradual dose escalation to a target of 0.5 mg/kg of each compound every 12 hours. The same formulation was applied topically to the wound once to twice daily. Treatment duration was 10 months, with concurrent multimodal analgesia as needed.
Cannabinoid therapy was associated with sustained improvements in appetite, body condition, pain, and mobility. Marked wound improvement was observed, including reduced granulation tissue, improved epithelialization, and resolution of self-mutilation.
No clinically relevant adverse effects or laboratory abnormalities occurred during routine dosing. Transient ataxia and sedation were noted only at high rescue doses near end of life. Despite eventual disease progression and euthanasia due to refractory pain, quality of life was substantially improved for most of the treatment period.
This case supports the potential role of combined THC-rich and CBD-rich cannabis oils as a safe and effective adjunct in multimodal palliative care for horses with chronic, refractory conditions. Controlled studies are warranted to define optimal dosing and indications.”
“Across veterinary species, cannabinoids have shown therapeutic potential with favorable safety and tolerability profiles.”
“The aim of this case report is to describe a long-term multimodal clinical approach using cannabinoids (THC and CBD) in a rescued horse affected by a wound/sarcoid and joint disease, as part of a palliative care strategy for pain management, inflammation control, and wound-healing enhancement.”
“This case suggests that long-term administration of THC-rich and CBD-rich cannabis oils may be a useful adjunct for palliative management in horses with chronic, refractory conditions.”
“Cannabinoid therapy was associated with improved comfort, mobility, and quality of life, supporting its potential role within multimodal palliative care.”
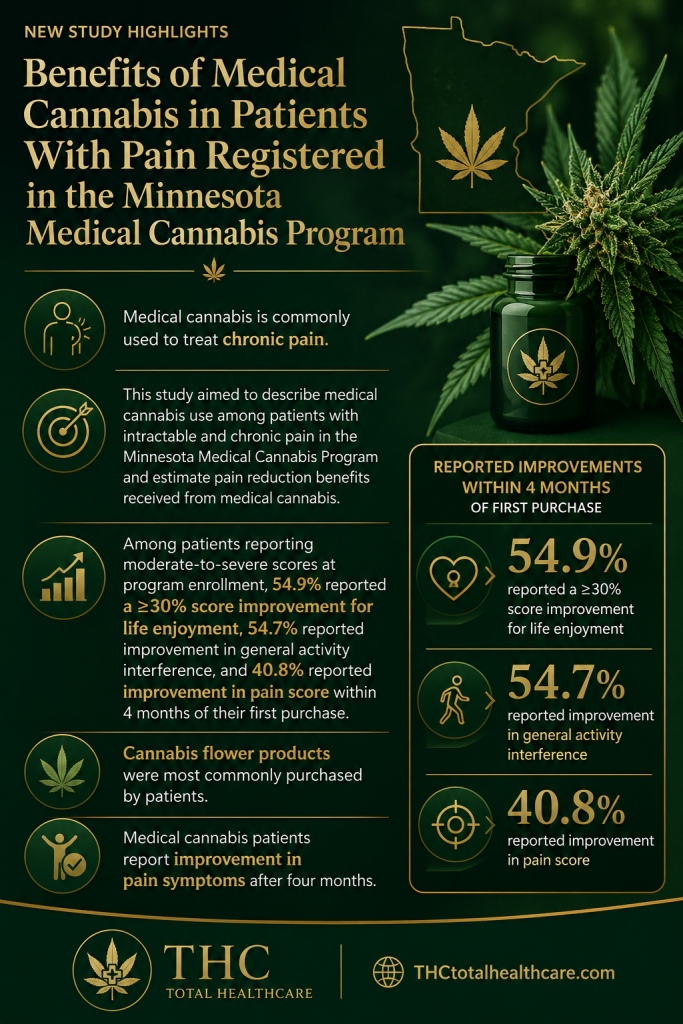
“Purpose: Medical cannabis is commonly used to treat chronic pain. Clinical trials typically use only one type and dosage of medical cannabis product, which is not reflective of real-world use. The use of a state-run medical cannabis program can bridge the gap between clinical research and real-world use of medical cannabis to estimate the benefits of cannabis use on patient symptoms. This study aimed to describe medical cannabis use among patients with intractable and chronic pain in the Minnesota Medical Cannabis Program and estimate pain reduction benefits received from medical cannabis.
Methods: Patients who enrolled in the Minnesota Medical Cannabis Program between March 2022 and February 2023 for chronic pain and purchased medical cannabis for at least 8 months were included in this study. Patients were required to complete the Patient Self-Evaluation before each medical cannabis purchase, which included the PEG (Pain, Enjoyment of Life, and General Activity) scale. The main outcome of this analysis was a ≥30% change in PEG component score within 4 months of first medical cannabis purchase. The proportion of patients who maintained that reduction for an additional 4 months was also calculated. Medical cannabis product purchases were queried from the first 4 months in the program and categorized by route of administration and tetrahydrocannabinol:cannabidiol ratio. Medical cannabis purchasing profiles were created using k-means clustering to group patients who purchased similar proportions of product types. Adjusted logistic regression models were run to investigate the association between medical cannabis purchasing profile and reporting ≥30% reduction in PEG score.
Findings: Among patients reporting moderate-to-severe scores at program enrollment, 54.9% reported a ≥30% score improvement for life enjoyment, 54.7% reported improvement in general activity interference, and 40.8% reported improvement in pain score within 4 months of their first purchase. Cannabis flower products were most commonly purchased by patients. High tetrahydrocannabinol:cannabidiol products were the most commonly purchased in all medical cannabis product categories. K-means clustering created 5 product purchasing profiles, which were not associated with PEG score improvement outcomes after adjustment for number of purchasing transactions.
Implications: Medical cannabis patients report reduction in PEG scores within 4 months of first medical cannabis purchase using a variety of medical cannabis products. Future research on medical cannabis should determine the frequency of use of different products and administration methods to further investigate how cannabis can be used for effective pain management in patients with chronic pain.”
“Introduction: Opioid use disorder (OUD) and chronic pain remain major global health challenges. Although opioid-based therapies provide effective analgesia, their long-term use is limited by safety concerns, dependence, and variable efficacy. Modulation of the endocannabinoid system (ECS) has emerged as a promising therapeutic strategy for pain management and opioid-related disorders.
Areas covered: This narrative review summarizes current evidence on ECS-targeted interventions for OUD, chronic non-cancer pain, and cancer-related pain. Relevant literature was identified through PubMed using search terms related to the ECS, cannabinoid receptors (CB1 and CB2), phytocannabinoids (Δ9 -tetrahydrocannabinol [THC] and cannabidiol [CBD]), synthetic cannabinoids, fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL) inhibitors, and opioid – cannabinoid interactions. Particular emphasis is placed on mechanistic interactions between ECS and opioid signaling pathways, as well as evidence from preclinical and clinical studies evaluating therapeutic efficacy and safety.
Expert opinion: ECS modulation may alleviate pain, reduce opioid withdrawal symptoms, and improve affective outcomes. Interactions between cannabinoid and opioid receptors may produce synergistic analgesic effects while potentially mitigating opioid tolerance and dependence. However, clinical translation remains limited by small sample sizes, heterogeneous study populations, and variability in trial design. Well-controlled clinical trials are needed to establish optimal dosing strategies, evaluate long-term safety, and clarify the therapeutic role of ECS-targeted interventions in OUD and pain management.”
“The endocannabinoid system (ECS) represents a promising therapeutic target for opioid use disorder (OUD), chronic non-cancer pain, and cancer-related pain.”
“Cannabinoids (e.g., CBD and Δ9 -THC) exert analgesic and anti-inflammatory effects through CB1-mediated central mechanisms and CB2-mediated peripheral mechanisms.”