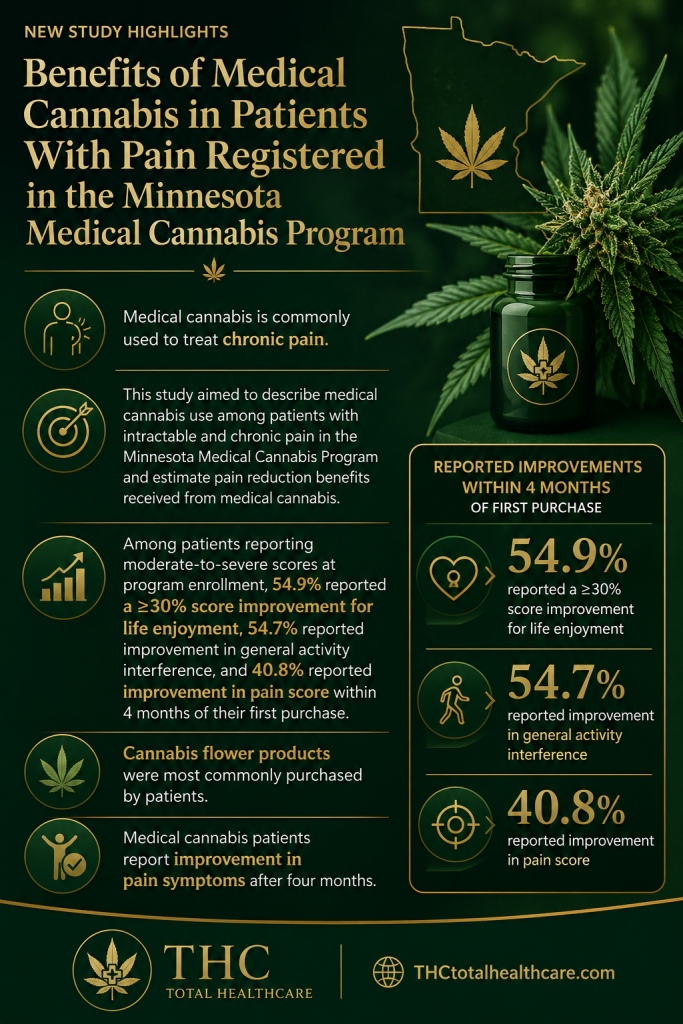
“Cannabinoid-based therapies have shown analgesic, anti-inflammatory, and wound-healing potential across veterinary species; however, clinical data on long-term use of THC-rich formulations in horses remain scarce.
This case report describes the use of combined oral and topical THC-rich and CBD-rich full-spectrum cannabis oils as part of a palliative care strategy in a rescued horse with severe chronic disease.
A senior mixed-breed gelding was rescued with a large, chronic ulcerative lesion of the left hind limb, severe malnutrition, non-weight-bearing lameness (AAEP grade 5/5), and refractory pain. Diagnostic workup identified a fibroblastic equine sarcoid complicated by complete suspensory tendon rupture, early osteomyelitis, and chronic joint disease. Conventional medical and surgical options were limited due to poor response, disease severity, and resource constraints.
A long-term palliative protocol was initiated using oral THC-rich and CBD-rich full-spectrum cannabis oils (1:1 ratio; 100 mg/mL each) with gradual dose escalation to a target of 0.5 mg/kg of each compound every 12 hours. The same formulation was applied topically to the wound once to twice daily. Treatment duration was 10 months, with concurrent multimodal analgesia as needed.
Cannabinoid therapy was associated with sustained improvements in appetite, body condition, pain, and mobility. Marked wound improvement was observed, including reduced granulation tissue, improved epithelialization, and resolution of self-mutilation.
No clinically relevant adverse effects or laboratory abnormalities occurred during routine dosing. Transient ataxia and sedation were noted only at high rescue doses near end of life. Despite eventual disease progression and euthanasia due to refractory pain, quality of life was substantially improved for most of the treatment period.
This case supports the potential role of combined THC-rich and CBD-rich cannabis oils as a safe and effective adjunct in multimodal palliative care for horses with chronic, refractory conditions. Controlled studies are warranted to define optimal dosing and indications.”
https://pubmed.ncbi.nlm.nih.gov/42311392
“Across veterinary species, cannabinoids have shown therapeutic potential with favorable safety and tolerability profiles.”
“The aim of this case report is to describe a long-term multimodal clinical approach using cannabinoids (THC and CBD) in a rescued horse affected by a wound/sarcoid and joint disease, as part of a palliative care strategy for pain management, inflammation control, and wound-healing enhancement.”
“This case suggests that long-term administration of THC-rich and CBD-rich cannabis oils may be a useful adjunct for palliative management in horses with chronic, refractory conditions.”
“Cannabinoid therapy was associated with improved comfort, mobility, and quality of life, supporting its potential role within multimodal palliative care.”
https://www.frontiersin.org/journals/veterinary-science/articles/10.3389/fvets.2026.1794084/full