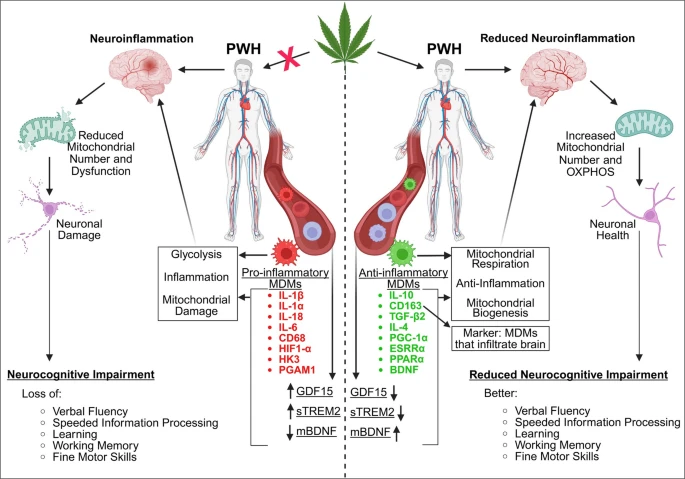
“CD16+ monocytes are a minor subset of the total monocyte population that play a disproportionate role in contributing to neuroinflammation in human immunodeficiency virus (HIV)-associated neurocognitive disorders (HAND).
This has been evidenced by the enhanced transmigration of CD16+ monocytes into the brain compared to their CD16– counterpart. CD16+ monocytes can be activated by HIV ssRNAs through toll-like receptors (TLR) 7 and TLR8, and subsequently interact with brain-resident cells, including astrocytes. Previous studies from our laboratory identified monocyte-derived IL-1ß as an inducing cytokine for astrocyte-derived neuroinflammatory factors.
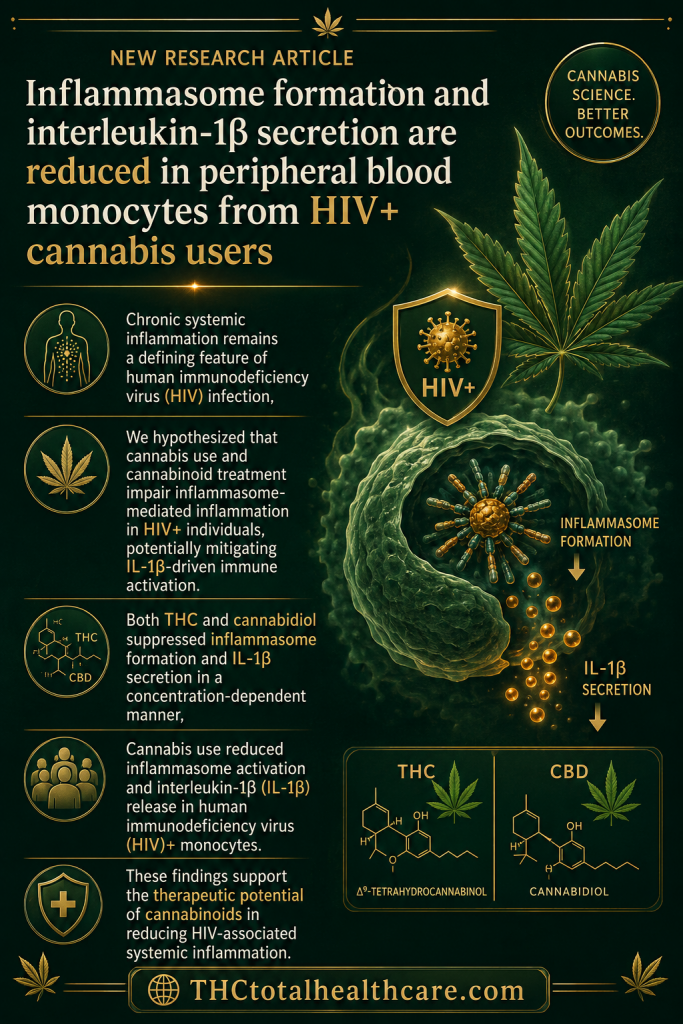
Despite cannabis use among the HIV community, the mechanisms by which immune-modulating cannabinoids, Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD), alter human immune responses in the context of HAND-associated neuroinflammation remain elusive.
We hypothesized that THC and CBD suppress CD16+ monocyte-induced astrocyte secretion of inflammatory mediators and monocyte recruitment via chemotaxis in the context of HIV.
Results from this study show that THC and CBD impair CD16+ monocyte IL-1ß-mediated astrocyte production of IL-6, IL-8, and MCP-1 when these two cell types are cocultured in the presence of TLR7 or TLR8 stimulation. Additionally, monocytes from HIV+ subjects exhibited enhanced migration compared to monocytes from HIV- subjects, which was suppressed by THC treatment but not by CBD. The effects on migration were associated with reduced cellular expression of polymerized actin and high-affinity conformation integrin receptors.
Collectively, these findings suggest that THC, and to a lesser extent CBD, may have therapeutic potential for mitigating CD16+ monocyte-mediated neuroinflammation associated with HAND.”
https://pubmed.ncbi.nlm.nih.gov/42400870
“Taken together, this study provides evidence to support that THC, and to a lesser extent CBD, exert anti-inflammatory effects on CD16+ monocyte-mediated inflammatory and migratory responses that may be associated with HAND.”
https://link.springer.com/article/10.1007/s11481-026-10300-2