“Traumatic brain injury (TBI) can cause severe neurological damage. Ferroptosis, a recently discovered form of iron-regulated cell death, is closely associated with TBI.
Cannabidiol (CBD) has been demonstrated to exhibit neuroprotective effects. However, the antiferroptotic role of CBD in TBI remains unclear. Investigating whether CBD inhibits ferroptosis after brain injury and its underlying mechanisms is of great significance.
We find that ferroptosis can be induced in rats after TBI, and CBD significantly inhibits ferroptosis in TBI rats both in vivo and in vitro.
MicroRNAs (miRNAs) are highly expressed in the brain. Differentially expressed miRNAs and mRNAs after TBI are detected by RNA sequencing, and miR-320-3p, Negr1, and the ERK/MEK pathway are screened out due to their strong correlations.
The results show that CBD inhibits miR-320-3p expression, increases Negr1 expression, and suppresses the ERK/MEK pathway both in vivo and in vitro. Mechanistically, transfection with miR-320-3p mimics or siNegr1 inhibits the intervention effect of CBD on ferroptosis and the ERK/MEK pathway. Additionally, Negr1 gene silencing reverses the effect of the miR-320-3p inhibitor on ferroptosis factors in PC12 cells, which suggests that miR-320-3p can target Negr1.
In conclusion, our findings indicate that CBD can inhibit TBI-induced ferroptosis through the miR-320-3p/Negr1/ERK signaling axis.”
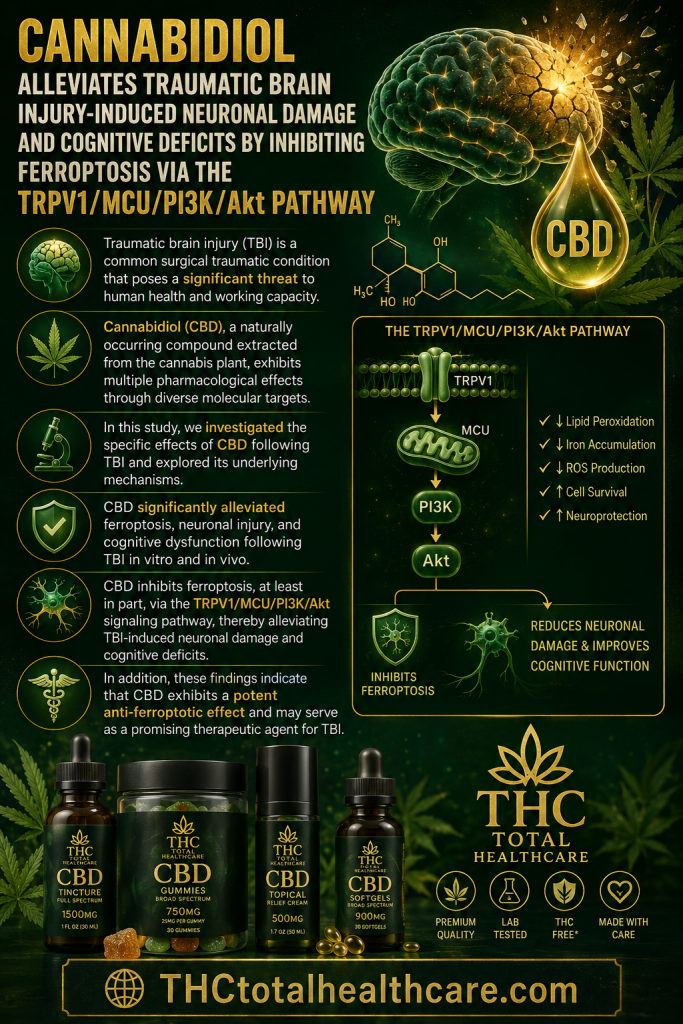
“Background: Traumatic brain injury (TBI) is a common surgical traumatic condition that poses a significant threat to human health and working capacity. However, effective treatments to improve its prognosis remain limited. Cannabidiol (CBD), a naturally occurring compound extracted from the cannabis plant, exhibits multiple pharmacological effects through diverse molecular targets. To date, the role and underlying molecular mechanisms of CBD in the context of TBI have not been fully elucidated. In this study, we investigated the specific effects of CBD following TBI and explored its underlying mechanisms.
Methods: An in vitro ferroptosis model was established using HT-22 cells, and an in vivo TBI model was established in mice. Techniques such as Western blotting, immunofluorescence staining, and behavioral analysis were employed to evaluate the effects of CBD on ferroptosis, pathological changes, and neurological function after TBI, as well as to explore the associated molecular mechanisms.
Results: CBD significantly alleviated ferroptosis, neuronal injury, and cognitive dysfunction following TBI in vitro and in vivo. Further investigation revealed that CBD mitigated mitochondrial dysfunction by reducing Ca2⁺ overload via the TRPV1/MCU signaling pathway. Moreover, utilizing methodologies such as recombinant adeno-associated virus (rAAV) injection and transcriptome analysis, mitochondrial calcium uniporter (MCU) was identified as a core regulator of ferroptosis in neurons following TBI. Neuronal MCU knockdown attenuated the progression of ferroptosis and improved neurological outcomes after TBI. Finally, integrated findings confirmed that CBD inhibit ferroptosis after TBI through the TRPV1/MCU/PI3K/Akt signaling pathway.
Conclusions: CBD inhibits ferroptosis, at least in part, via the TRPV1/MCU/PI3K/Akt signaling pathway, thereby alleviating TBI-induced neuronal damage and cognitive deficits. In addition, these findings indicate that CBD exhibits a potent anti-ferroptotic effect and may serve as a promising therapeutic agent for TBI.”
“Background: Paroxysmal Sympathetic Hyperactivity (PSH) is a well-recognized complication following severe traumatic brain injury (TBI), with an incidence of 5-33% in the acute phase, characterized by episodic autonomic and motor hyperactivity. Management is often challenging, and a subset of patients develop refractory PSH despite optimized first- and second-line therapies. Cannabidiol (CBD) possesses neuroregulatory and autonomic-modulating properties demonstrated in preclinical TBI studies and epilepsy trials including Epidiolex studies, but its role in PSH has not been previously described.
Case presentation: We report the case of a 44-year-old South Indian gentleman with severe TBI following a road traffic accident (GCS 5: E1V1M3) with CT brain showing bilateral frontotemporo-parietal acute subdural hematoma with mass effect. He underwent emergency bilateral decompressive craniectomy and required mechanical ventilation with tracheostomy. Three weeks post-injury, he developed recurrent PSH episodes (4-6 episodes per day) characterized by severe tachycardia (heart rate 140-180 bpm), hypertension (systolic blood pressure > 180 mmHg), hyperthermia (up to 40 °C), diaphoresis, and dystonic posturing. The diagnosis of PSH was established using the Paroxysmal Sympathetic Hyperactivity Assessment Measure (PSH-AM), with a total score of 28 (Clinical Feature Scale: 18, Diagnosis Likelihood Tool: 10), indicating probable PSH. Infective, metabolic, epileptic, and structural causes were excluded. Despite treatment with multiple conventional agents at maximum tolerated doses-including bromocriptine (titrated from 1.25 mg twice daily to 40 mg/day), baclofen (10 mg/day), gabapentin (titrated from 150 mg/day to 300 mg/day), propranolol (15 mg three times daily), clonidine (0.2 mg/day), dexmedetomidine infusion (72-h infusion), and fentanyl (infusion followed by patches)-the autonomic storms persisted, fulfilling criteria for refractory PSH.
Cannabidiol oil (100 mg/mL) was therefore initiated as adjunctive therapy at 100 mg twice daily (approximately 3 mg/kg/day) and titrated to a 100-150-100 mg/day regimen over one week via nasogastric tube. Within the first week, there was a marked reduction in episode frequency (from 4 to 6 per day to less than 1 per 48 h) and severity, with PSH-AM scores decreasing from 28 (CFS: 18, DLT: 10) to 16 (CFS: 6, DLT: 10), and opioid and sedative infusions were successfully withdrawn. By the second week, complete resolution of PSH episodes was achieved with a PSH-AM score of 4. No adverse effects were observed, including no hepatic dysfunction, excessive sedation, or hemodynamic instability.
Conclusions: This case highlights a potential adjunctive role for cannabidiol in refractory PSH following severe TBI. While causality cannot be inferred from a single observation, the sustained clinical improvement after failure of conventional therapies warrants further prospective investigation.”
“An optimal ratio of cannabidiol (CBD) to tetrahydrocanabinol (THC) was hypothesized to protect against neuropathological consequences following traumatic brain injury (TBI).
Varied CBD:THC extract concentrations were compared with hemp CBD lacking THC (CBD0). Neurons, glia, and parvalbumin interneurons (PV-INs) were evaluated.
Weight loss was observed following high doses of THC dominant cannabis, THC100:1. Neuroscores and vestibulomotor performance were restored most with CBD:THC300:1-10:1. However, THC dominant treatments resulted in early onset to spontaneous seizures post-TBI.
The alternating T-maze showed the CBD10:1 group had the highest spontaneous alternation rates whereas TBI + vehicle, CBD0, CBD1:1, and THC100:1 groups had the lowest. The novel object recognition memory task showed CBD300:1 treated animals had the best performance, while TBI or THC100:1 treated groups had the worst. The forced swim test (FST) revealed immobility time was highest after TBI and lowest after THC20:1 or THC100:1 treatment post-TBI. The elevated plus maze (EPM) revealed the CBD0 group spent the most time in closed arms. Both tests indicate that reduced anxiety was THC dependent. In the absence of TBI, THC20:1 treatment resulted in the highest mobility.
All combinations resulted in reduced injury post-TBI but CBD10:1 and THC20:1 afforded the most protection and THC100:1 the least. Reduced GFAP labeling was highest with CBD dominant cannabis supporting its neuroprotective role against inflammation. Rescue of diminished bilateral PV-INs was observed within the hippocampus and medial prefrontal cortex (mPFC) with CBD dominant treatment (CBD300, CBD0) supporting their anticonvulsant effect. Loss of PV-INs with THC dominant treatment supports their proconvulsant effect. Thus, CBD and THC have different beneficial therapeutic effects indicating an optimal concentration ratio is critical for neuropathological therapeutics.
SIGNIFICANCE STATEMENT: There is currently no optimal treatment that can prevent behavioral and cellular pathology as well as onset of spontaneous seizures associated with traumatic brain injury (TBI). We hypothesized that an optimal ratio of CBD:THC is required to protect against neuropathological consequences following TBI. Six extracts with varied CBD:THC ratio concentrations were compared with hemp CBD lacking THC. CBD dominant cannabis with critical THC dosing afforded the most neuroprotection and behavioral recovery, whereas THC dominant cannabis stimulated spontaneous seizure onset. CBD and THC had different beneficial therapeutic effects indicating an optimal concentration ratio is critical for neuropathological therapeutics. Absorbable medical carriers will offer delivery treatment options to optimize both short- and long-term drug efficacy relating to neuropathological disorders.”
“Background: Perinatal hypoxia-ischemia is a major cause of long-term neurological impairments in newborns, with ferroptosis recognized as a key mechanism of injury.
Cannabidiol (CBD) is a non-psychoactive phytocannabinoid with antioxidant and neuroprotective properties.
CBD is a potential modulator of hypoxic-ischemic brain damage, however its effects on ferroptosis-related pathways remain unclear.
Purpose: In this study, we examined whether CBD can alleviate ferroptosis-associated damage in differentiated human neuroblastoma (neuron-like SH-SY5Y) cell model of hypoxic-ischemic injury.
Study design: Differentiated human neuroblastoma cells were exposed to oxygen-glucose deprivation (OGD) to simulate hypoxic-ischemic conditions.
Methods: Neuron-like SH-SY5Y cells were subjected to OGD to induce hypoxic-ischemic injury. CBD was applied to assess its neuroprotective effects. Oxidative stress markers, antioxidant enzyme activity, transcription factor activation Nrf2 (nuclear factor erythroid 2-related factor 2), iron metabolism proteins (ferroportin), hypoxia-inducible factor 1 alpha (HIF-1α) and vascular endothelial growth factor (VEGF) expression were evaluated.
Results: CBD application significantly reduced oxidative stress by improving antioxidant capacity and lowering total oxidant status. CBD also preserved the expression and enzymatic activity of glutathione peroxidase 4, a central enzyme protecting against lipid peroxidation, and enhanced the activation of Nrf2, a key regulator of antioxidant defence. Additionally, CBD prevented OGD-induced downregulation of ferroportin, potentially supporting iron efflux and reducing ferroptotic risk. HIF-1α and its downstream target VEGF were upregulated under hypoxic conditions, and CBD further enhanced VEGF expression.
Conclusion: CBD mitigates ferroptosis by modulating redox balance, antioxidant defence, and iron metabolism, supporting its potential role as a therapeutic strategy for neonatal hypoxic-ischemic brain injury.”
“These findings support the potential use of CBD as a therapeutic agent for hypoxia-related ferroptotic injury, such as neonatal hypoxic-ischemic encephalopathy.”
“Background: Cognitive impairment is a major complication of traumatic brain injury (TBI), yet effective therapies remain lacking. As a natural compound extracted from Cannabis sativa, cannabidiol (CBD) possesses antioxidant properties and has shown neuroprotective potential in several neurological disorders. However, its effects in cognitive impairment after TBI remain unclear.
Purpose: This study aimed to investigate the therapeutic effects of CBD on cognitive impairment after TBI and elucidate its underlying molecular mechanisms.
Study design: In vitro H2O2 model and in vivo TBI model were used to evaluate the neuroprotective effects of CBD.
Methods: Neuronal oxidative stress models induced by H2O2 and controlled cortical impact model were used to detect the neuroprotective effects of CBD. Western blotting, histological staining, and biochemical assays were employed to investigate the effects of CBD on oxidative stress and apoptosis in neurons. RNA-Seq analysis, co-immunoprecipitation, molecular dynamics simulations, CETSA, SPR and immunofluorescence were performed to elucidate the molecular mechanisms.
Results: CBD can inhibit neuronal oxidative stress and apoptosis both in vivo and in vitro. Mechanistically, we identify a novel SET/PP2A/Akt signaling axis, in which CBD directly bound to SET, induced conformational changes in its nuclear localization signal and promoted its retention in the cytoplasm. Elevated cytoplasmic SET suppresses PP2A activity, activates Akt signaling pathway, and inhibits oxidative stress and pro-apoptotic cascades, promoting neuronal survival.
Conclusion: CBD exerts its neuroprotective effects by inhibiting neuronal oxidative stress and apoptosis through SET/PP2A/Akt signaling axis. These findings provide a novel potential drug target for the treatment of cognitive impairment after TBI.”
“Cannabidiol alleviates cognitive impairment after traumatic brain injury in mice.”
“This work not only enhances understanding of post-TBI pathophysiology but also provides mechanistic insights supporting the potential clinical application of CBD in post-TBI cognitive impairment.”
“Hypothesis: Administration of the phytocannabinoid Δ9-tetrahydrocannabinol (Δ9-THC) will enhance brain repair and improve short-term spatial working memory in mice following controlled cortical impact (CCI) by upregulating granulocyte colony-stimulating factor (G-CSF) and other neurotrophic factors (brain-derived neurotrophic factor [BDNF], glial-derived neurotrophic factor [GDNF]) in hippocampus (HP), cerebral cortex, and striatum.
Materials and Methods: C57BL/6J mice underwent CCI and were treated for 3 days with Δ9-THC 3 mg/kg intraperitoneally (i.p.). Short-term working memory was determined using the spontaneous alternations test during exploratory behavior in a Y-maze. Locomotor function was measured as latency to fall from a rotating drum (rotometry). These behaviors were recorded at baseline and 3, 7, and 14 days after CCI. Groups of mice were euthanized at 7 and 14 days. Extent of microgliosis, astrocytosis, and G-CSF, BDNF, and GDNF expression were measured at 7 and 14 days in cerebral cortex, striatum, and HP on the side of the trauma. Levels of the most abundant endocannabinoid (2-arachidonoyl-glycerol [2-AG]) was also measured at these times.
Results: Δ9-THC-treated mice exhibited marked improvement in performance on the Y-maze indicating that treatment with the phytocannabinoid could reverse the deficit in working memory caused by the CCI. Δ9-THC-treated mice ran on the rotarod longer than vehicle-treated mice and recovered to normal rotarod performance levels at 2 weeks. Δ9-THC-treated mice, compared with vehicle-treated animals, exhibited significant upregulation of G-CSF as well as BDNF and GDNF in the cerebral cortex, striatum, and HP. Levels of 2-AG were also increased in the Δ9-THC-treated mice.
Conclusion: Administration of the phytocannabinoid Δ9-THC promotes significant functional recovery from traumatic brain injury (TBI) in the realms of working memory and locomotor function. This beneficial effect is associated with upregulation of brain 2-AG, G-CSF, BDNF, and GDNF. The latter three neurotrophic factors have been previously shown to mediate brain self-repair following TBI and stroke.”
“Oral administration of drugs in laboratory rodents such as rats is conventionally performed using the gavage technique. Despite effectiveness, gavage can induce distress associated with restraint, especially following repeated animal handling.
To mitigate these adverse effects and reduce morbidity associated with traditional methods, we explored oromucosal/buccal administration of cannabidiol (CBD)-enriched Cannabis extract.
In this method, male rats were treated daily for 15 days with medium-chain triglycerides (TCM) derived from coconut oil or CBD-enriched Cannabis extract. Each treatment was administered individually while animals were gently immobilized using an affectionate touch technique. The administration involved the use of a micropipette to apply the oily formulation directly into the oral mucosa. The dosage was calculated based on the CBD concentration in the Cannabis extract, standardized at 3 mg/kg/day. To ensure accuracy, animals were weighed daily, allowing for dose adjustments in accordance with weight changes over the treatment period. This method offers non-invasive and stress-reducing treatment, potentially improving animal welfare in experimental settings.
The treatment with CBD-enriched Cannabis extract was safe, and the analysis of the hippocampus of these animals’ showed alterations in the expression levels of GluA1 and GFAP proteins, which are directly associated with glutamatergic receptor functionality and neuroinflammation, respectively. This suggests that Cannabis extract could be applied in pathological conditions where glutamatergic excitotoxicity and astrogliosis are observed.”
“Objectives: To explore the effects of cannabidiol on endoplasmic reticulum stress and neuronal apoptosis in rats with multiple concussions (MCC).
Methods: SD rats were randomized into sham group, MCC group, 1% tween20 (TW) treatment group, and low-dose (10 mg/kg) and high-dose (40 mg/kg) cannabidiol treatment groups. In all but the sham group, MCC models were established using a metal pendulum percussion device, after which the rats received daily intraperitoneal injections of the corresponding agents for 2 weeks. The expressions of PERK, eIF2α, ATF4, CHOP, TRIB3, p-Akt and pro-caspase-3 in the brain tissue of the rats were detected with qRT-PCR, Western blotting and immunofluorescence staining. The core targets of cannabidiol in treatment of traumatic brain injury (TBI) were identified by network pharmacology analysis, and molecular docking was carried out to simulate the interaction of cannabidiol with the factors related to endoplasmic reticulum stress and apoptosis.
Results: Compared with the sham-operated rats, the rat models of MCC showed significantly increased mRNA expressions of PERK, eIF2α and CHOP and protein expressions of PERK, eIF2α, ATF4, CHOP, TRIB3, p-AKT and pro-caspase-3 in the cerebral cortex. CBD treatment, especially at the high dose, obviously increased the expression of p-Akt and lowered the expression levels of the other factors tested in the rat models. Network pharmacology analysis indicated interactions of the core targets of CBD with the factors related to endoplasmic reticulum stress and TBI, and molecular docking study showed a high binding energy of CBD with multiple factors pertaining to endoplasmic reticulum stress and apoptosis.
Conclusions: MCC induce endoplasmic reticulum stress and apoptosis in rat brain tissues, for which CBD, especially at a high dose, provides neuroprotective effects by inhibiting endoplasmic reticulum stress and cell apoptosis.”
“Ethnopharmacological relevance: Posttraumatic epilepsy (PTE) is an acquired epilepsy caused by traumatic brain injury (TBI). From Mesopotamian civilization to Eastern medical classics, the use of Cannabis for anticonvulsant purposes has spanned three millennia of medical history. As a non-psychoactive plant extract of Cannabis, cannabidiol (CBD) has attracted considerable attention in epilepsy-related treatment. However, whether CBD exhibits an anticonvulsant effect against PTE and its underlying molecular mechanisms remains to be elucidated.
Aim of the study: This study aims to investigate the anticonvulsant and neuroprotective effect of CBD on PTE, as well as its molecular mechanisms.
Methods: Ferric chloride (FeCl3)-induced PTE rat models were constructed in normal rats and brain-localized transient receptor potential vanilloid type 1 (TRPV1) overexpression rats. The anticonvulsant effects of CBD were evaluated by epileptic behavioral scoring and electroencephalogram (EEG) monitoring. The neuroprotective effect was measured by histopathological staining of the brain tissues. Immunofluorescence, western blot, q-PCR and Ca2+ fluorescence intensity detection were employed to investigate the mechanisms of CBD on PTE rats.
Results: CBD significantly reduced the seizure severity and brain damage in FeCl3-induced PTE rat models. Besides, EEG data showed decreased amplitude, total power, and spike wave discharges in PTE rats pretreated with CBD. Moreover, CBD suppressed the phosphorylation of heat shock factor 1 (HSF1) by targeting TRPV1, thereby specifically inhibiting the stress-induced heat shock protein 70 (HSP70) increase in the brain-localized TRPV1 overexpression rats.
Conclusion: CBD exerts an anticonvulsant and neuroprotective effect on PTE rats by regulating the TRPV1/HSF1/HSP70 pathway and may be a potential drug for the prophylactic treatment of PTE.”