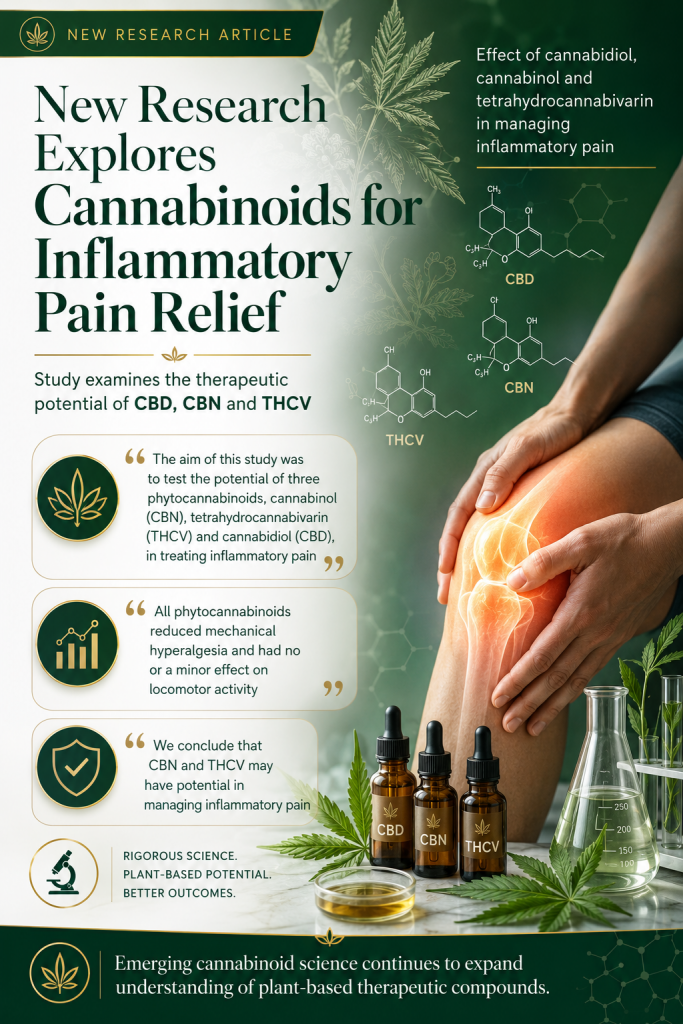
Background: Chronic neuropathic pain (NP) is frequently accompanied by anxiety- and depression‑like symptoms, reflecting maladaptive interactions between nociceptive and affective brain networks. The anterior insular cortex (AIC) integrates sensory and emotional dimensions of pain and represents a potential target for pharmacological modulation. Cannabidiol (CBD) exhibits analgesic and anxiolytic/antidepressant‑like properties through interactions with endocannabinoid and serotonergic systems.
Objectives: We investigated whether CBD microinjection into the AIC modulates NP and its affective comorbidities, and whether these effects depend on CB1 and 5‑HT1A receptors.
Methods: Male Wistar rats were subjected to chronic constriction injury (CCI) of the sciatic nerve. Fourteen days later, guide cannulae were implanted into the AIC. On day 21 post‑CCI, animals received intra‑AIC microinjections of CBD (15, 30, or 60 nmol/200 nL) or vehicle. Mechanical (von Frey test) and cold (acetone test) allodynia, anxiety‑like behavior (open field and elevated plus maze tests), and depression‑like behavior (forced swim and sucrose spray tests) were assessed by different psychobiological tests. The role of cannabinoid and serotonergic receptors was addressed by intra‑AIC pretreatment with either the CB1 receptor antagonist AM251 or the 5‑HT1A receptor antagonist WAY-100,635 in independent groups.
Results: AIC pretreatment with CBD dose‑dependently reduced mechanical and cold allodynia and anxiety‑ and depression‑like behaviors, with the most robust effects observed at 60 nmol. AIC Pretreatment with either AM251 or WAY-100,635 abolished the antinociceptive and affective effects of CBD.
Conclusion: CBD administration within the AIC produces integrated analgesic, anxiolytic, and antidepressant-like effects in a model of neuropathic pain. These effects are consistent with the involvement of CB1 and 5-HT1A receptor signaling. The findings identify the AIC as a relevant cortical substrate linking nociceptive and affective processes and support CBD as a promising psychopharmacological strategy for NP associated with emotional comorbidities.”
https://pubmed.ncbi.nlm.nih.gov/42390818
“In conclusion, this study demonstrates that CBD microinjection into the AIC attenuates mechanical and cold allodynia while also reducing anxiety- and depression-like behaviors in an experimental model of NP.”
“Overall, these findings highlight the AIC as a potential neural substrate involved in the interaction between chronic pain and its emotional comorbidities and identify CBD as a promising psychopharmacological approach for NP conditions associated with affective dysfunction.”
https://link.springer.com/article/10.1007/s00213-026-07116-6