“Chronic pain is highly prevalent and inadequately managed by current therapeutic strategies, which present significant limitations such as the development of tolerance, dependence, and cognitive impairment. Therefore, searching for new pain management strategies is an ultimate goal.
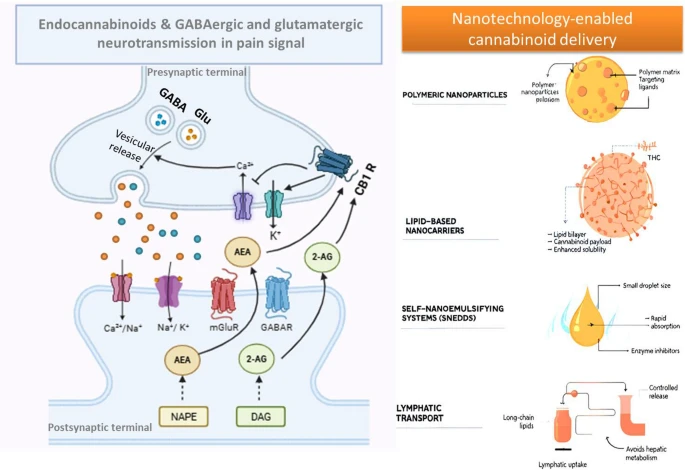
The endocannabinoid system (ECS), is a broad crucial regulatory network in central nervous system’s development and in modulating various physiological and cognitive functions. It comprises endogenous cannabinoids, cannabinoid receptors, and the enzymes governing cannabinoid production and breakdown.
Recently, cannabinoids, particularly medical cannabis, have garnered renewed interest for their possibilities in treating different medical conditions, including chronic pain.
Although the risk of lethal overdose is negligible, the prevalence of non-serious adverse effects is significant and requires careful clinical consideration. Currently, there is a paucity of sufficient efficacy and long-term safety data to fully support the systematic use of medical cannabis for chronic non-malignant pain conditions.
Further research is crucial to unlock the future potential of these approaches and to delineate essential directions for exploring the ECS and its role in pain management. Advances in nanotechnology have enabled novel delivery platforms that address key limitations of cannabinoid-based therapies.
Nanocarriers, including lipid and polymeric nanoparticles, nanoemulsions, and self-emulsifying systems, can improve cannabinoid solubility, stability, bioavailability, and targeted delivery. Through controlled release and site-specific targeting, these systems hold promise for enhancing the analgesic efficacy and safety of cannabinoid therapeutics.”
https://pubmed.ncbi.nlm.nih.gov/42154330
https://link.springer.com/article/10.1007/s11011-026-01862-4