“Cannabis sativa L. (Cannabis) and its bioactive compounds, including cannabinoids and non-cannabinoids, have been extensively studied for their biological effects in recent decades. Cannabidiol (CBD), a major non-intoxicating cannabinoid in Cannabis, has emerged as a promising intervention for cancer research.
The purpose of this review is to provide insights into the relationship between CBD and cancer based on recent research findings.
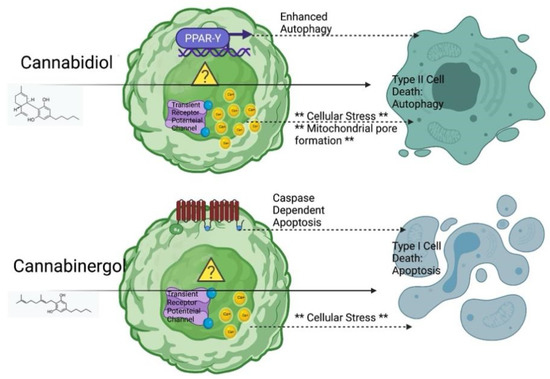
The anticancer effects of CBD are mainly mediated via its interaction with the endocannabinoid system, resulting in the alleviation of pain and the promotion of immune regulation. Published reviews have focused on the applications of CBD in cancer pain management and the possible toxicological effects of its excessive consumption.
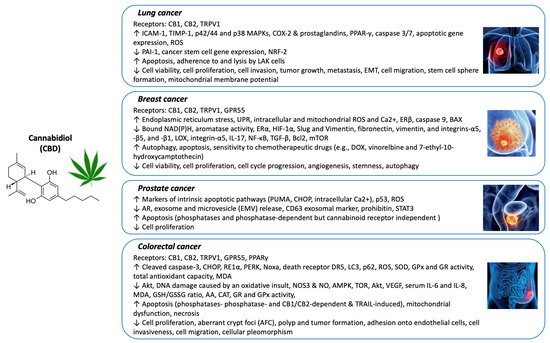
In this review, we aim to summarize the mechanisms of action underlying the anticancer activities of CBD against several common cancers. Studies on the efficacy and mechanisms of CBD on cancer prevention and intervention in experimental models (i.e., cell culture- and animal-based assays) and human clinical studies are included in this review.”
https://pubmed.ncbi.nlm.nih.gov/35741337/
“Emerging evidence suggests positive outcomes from the use of CBD as a cancer treatment. CBD can relieve cancer pain and ease the side effects of chemotherapy; however, there is less research about the mechanism of CBD’s anticancer effects. In this article, recent studies on the efficacy and mechanisms of CBD’s anticancer effects in cell- and animal-based models and human clinical studies are reviewed.”
https://www.mdpi.com/2079-7737/11/6/817