
![]() “Grade IV glioblastoma multiforme is a deadly disease, with a median survival of around 14 to 16 months. Maximal resection followed by adjuvant radiochemotherapy has been the mainstay of treatment since many years, although survival is only extended by a few months. In recent years, an increasing number of data from in vitro and in vivo research with cannabinoids, particularly with the non-intoxicating cannabidiol (CBD), point to their potential role as tumour-inhibiting agents. Herein, a total of nine consecutive patients with brain tumours are described as case series; all patients received CBD in a daily dose of 400 mg concomitantly to the standard therapeutic procedure of maximal resection followed by radiochemotherapy. By the time of the submission of this article, all but one patient are still alive with a mean survival time of 22.3 months (range=7-47 months). This is longer than what would have been expected.”
“Grade IV glioblastoma multiforme is a deadly disease, with a median survival of around 14 to 16 months. Maximal resection followed by adjuvant radiochemotherapy has been the mainstay of treatment since many years, although survival is only extended by a few months. In recent years, an increasing number of data from in vitro and in vivo research with cannabinoids, particularly with the non-intoxicating cannabidiol (CBD), point to their potential role as tumour-inhibiting agents. Herein, a total of nine consecutive patients with brain tumours are described as case series; all patients received CBD in a daily dose of 400 mg concomitantly to the standard therapeutic procedure of maximal resection followed by radiochemotherapy. By the time of the submission of this article, all but one patient are still alive with a mean survival time of 22.3 months (range=7-47 months). This is longer than what would have been expected.”
Category Archives: Cancer
Targeting Cannabinoid 1 and Delta Opioid Receptor Heteromers Alleviates Chemotherapy-Induced Neuropathic Pain.

“Cannabinoid 1 (CB1R) and delta opioid receptors (DOR) associate to form heteromers that exhibit distinct pharmacological properties.
Not much is known about CB1R-DOR heteromer location or signaling along the pain circuit in either animal models or patients with chemotherapy-induced peripheral neuropathy (CIPN).
Here, we use paclitaxel to induce CIPN in mice and confirm the development of mechanical allodynia.
Together, these results imply that CB1R-DOR heteromers upregulated during CIPN-associated mechanical allodynia could serve as a potential target for treatment of neuropathic pain including CIPN.”
Altered mRNA Expression of Genes Involved in Endocannabinoid Signalling in Squamous Cell Carcinoma of the Oral Tongue.
 “Little is known about the endocannabinoid (eCB) system in squamous cell carcinoma of the oral tongue (SCCOT). Here we have investigated, at the mRNA level, expression of genes coding for the components of the eCB system in tumour and non-malignant samples from SCCOT patients. Expression of NAPEPLD and PLA2G4E, coding for eCB anabolic enzymes, was higher in the tumour tissue than in non-malignant tissue. Among genes coding for eCB catabolic enzymes, expression of MGLL was lower in tumour tissue while PTGS2 was increased. It is concluded that the eCB system may be dysfunctional in SCCOT.”
“Little is known about the endocannabinoid (eCB) system in squamous cell carcinoma of the oral tongue (SCCOT). Here we have investigated, at the mRNA level, expression of genes coding for the components of the eCB system in tumour and non-malignant samples from SCCOT patients. Expression of NAPEPLD and PLA2G4E, coding for eCB anabolic enzymes, was higher in the tumour tissue than in non-malignant tissue. Among genes coding for eCB catabolic enzymes, expression of MGLL was lower in tumour tissue while PTGS2 was increased. It is concluded that the eCB system may be dysfunctional in SCCOT.”
https://www.ncbi.nlm.nih.gov/pubmed/31423851
“There is good evidence that the eCB system is disrupted in cancer. The present study represents an initial investigation into the eCB system in SCCOT. In conclusion, the present study has shown that at the mRNA level, the eCB system is disturbed in SCCOT compared to non-malignant tongue tissue.”
Endocannabinoid system and the expression of endogenous ceramides in human hepatocellular carcinoma.
 “The endogenous lipid metabolism network is associated with the occurrence and progression of malignancies.
“The endogenous lipid metabolism network is associated with the occurrence and progression of malignancies.
Endocannabinoids and ceramides have demonstrated their anti-proliferative and pro-apoptotic properties in a series of cancer studies.
The aim of the present study was to evaluate the expression patterns of endocannabinoids and endogenous ceramides in 67 pairs of human hepatocellular carcinoma (HCC) tissues and non-cancerous counterpart controls.
Anandamide (AEA), the major endocannabinoid, was reduced in tumor tissues, probably due to the high expression and activity of fatty acid amide hydrolase. Another important endocannabinoid, 2-arachidonylglycerol (2-AG), was elevated in tumor tissues compared with non-tumor controls, indicating that the biosynthesis of 2-AG is faster than the degradation of 2-AG in tumor cells.
Furthermore, western blot analysis demonstrated that cannabinoid receptor 1 was downregulated, while cannabinoid receptor 2 was elevated in HCC tissues, in accordance with the alterations in the levels of AEA and 2-AG, respectively. For HCC tissues, the expression levels of C18:0, 20:0 and 24:0-ceramides decreased significantly, whereas C12:0, 16:0, 18:1 and 24:1-ceramides were upregulated, which may be associated with cannabinoid receptor activation and stearoyl-CoA desaturase protein downregulation.
The exact role of endocannabinoids and ceramides in regulating the fate of HCC cells requires further investigation.”
https://www.ncbi.nlm.nih.gov/pubmed/31423220
https://www.spandidos-publications.com/10.3892/ol.2019.10399
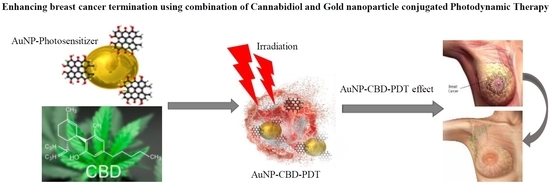
Enhancing Breast Cancer Treatment Using a Combination of Cannabidiol and Gold Nanoparticles for Photodynamic Therapy.
![]() “Indisputably, cancer is a global crisis that requires immediate intervention. Despite the use of conventional treatments over the past decades, it is acceptable to admit that these are expensive, invasive, associated with many side effects and, therefore, a reduced quality of life.
“Indisputably, cancer is a global crisis that requires immediate intervention. Despite the use of conventional treatments over the past decades, it is acceptable to admit that these are expensive, invasive, associated with many side effects and, therefore, a reduced quality of life.
One of the most possible solutions to this could be the use of gold nanoparticle (AuNP) conjugated photodynamic therapy (PDT) in combination with cannabidiol (CBD), a Cannabis derivative from the Cannabis sativa.
Since the use of Cannabis has always been associated with recreation and psychoactive qualities, the positive effects of Cannabis or its derivatives on cancer treatment have been misunderstood and hence misinterpreted.
On the other hand, AuNP-PDT is the most favoured form of treatment for cancer, due to its augmented specificity and minimal risk of side effects compared to conventional treatments. However, its use requires the consideration of several physical, biologic, pharmacologic and immunological factors, which may hinder its effectiveness if not taken into consideration.
In this review, the role of gold nanoparticle mediated PDT combined with CBD treatment on breast cancer cells will be deliberated.”
https://www.ncbi.nlm.nih.gov/pubmed/31561450
https://www.mdpi.com/1422-0067/20/19/4771
Cannabis use in cancer: a survey of the current state at BC Cancer before recreational legalization in Canada.
 “Cancer patients experience multiple symptoms throughout their illness, and some report benefit from the use of cannabis. There are concerns that many patients are accessing products inappropriate for their situation and potentially putting themselves at risk.
“Cancer patients experience multiple symptoms throughout their illness, and some report benefit from the use of cannabis. There are concerns that many patients are accessing products inappropriate for their situation and potentially putting themselves at risk.
In the present study, we aimed to capture the prevalence of cannabis use among cancer patients at BC Cancer before recreational legalization in Canada and to identify the reasons that patients take cannabis, the various routes of administration they use, and the reasons that prior users stopped.
RESULTS:
Of surveys sent to 2998 patients, 821 (27.4%) were returned and included in analysis. Of those respondents, 23% were currently using cannabis-based products, almost exclusively for medical purposes, and an additional 28% had been users in the past (most often recreationally). Of the patients currently using cannabis, 31% had medical authorization. The most common symptoms that the current users were targeting were pain, insomnia, nausea, and anxiety; many were also hoping for anticancer effects.
CONCLUSIONS:
More than half the respondents had tried cannabis at some time, and almost one quarter of respondents were currently taking cannabis to help manage their symptoms or treat their cancer, or both. Many more patients would consider use with appropriate guidance from a health care professional. More research is needed to inform physicians and patients about safe uses and doses and about the potential adverse effects of cannabis use.”
A Novel Highly Selective Cannabinoid CB2 Agonist Reduces in Vitro Growth and TGF-beta Release of Human Glial Cell Tumors.
 “Cannabinoid receptors have been detected in human gliomas and cannabinoids have been proposed as novel drug candidates in the treatment of brain tumors.
“Cannabinoid receptors have been detected in human gliomas and cannabinoids have been proposed as novel drug candidates in the treatment of brain tumors.
Aim of this study was to test the in vitro antitumor activity of COR167, a novel cannabinoid CB2-selective agonist displaying high binding affinity for human CB2 receptors, on tumor cells isolated from human glioblastoma multiforme and anaplastic astrocytoma.
RESULTS:
COR167 was found to significantly reduce the proliferation of both glioblastoma and anaplastic astrocytoma in a dose-dependent manner at lower doses than other known, less specific CB2 agonists. This activity is independent of apoptosis and is associated with significant reduction of TGF-beta 1 and 2 levels in supernatants of glioma cell cultures.
CONCLUSIONS:
These findings add to the role of cannabinoid CB2 receptor as a possible pharmacological target to counteract glial tumor growth and encourage further work to explore any other pharmacological effect of this novel CB2 agonist useful in the treatment of human gliomas.”
Antiproliferative and antioxidant effect of polar hemp extracts (Cannabis sativa L., Fedora cv.) in human colorectal cell lines.
 “Total phenolic content and antioxidant activity of polar extracts of edible resources from Fedora hemp cultivar (Cannabis sativa L.), namely seed, flour and oil, were evaluated. The main components in the polar extracts were identified using HPLC-DAD and HPLC-ESI-MS/MS. As expected, the molecular profile of components from seeds and flour was strictly similar, dominated by N-trans-caffeoyltyramine. The profile of oil polar extracts contained hydroxycinnamic acid derivatives and cannabinoids at lower extent. While the extracts from hemp seed and flour did not interfere with growth of Caco-2 and HT-29 cell, the one from oil (150 µg/mL) significantly reduced cell viability after 24 h of treatment. This effect was associated with the activation of apoptotic cell death and was independent from the antioxidant capacity of the oil polar extract. Notably, HT-29 cells differentiated with sodium butyrate were not sensitive to the cytotoxic effect of the oil extract.”
“Total phenolic content and antioxidant activity of polar extracts of edible resources from Fedora hemp cultivar (Cannabis sativa L.), namely seed, flour and oil, were evaluated. The main components in the polar extracts were identified using HPLC-DAD and HPLC-ESI-MS/MS. As expected, the molecular profile of components from seeds and flour was strictly similar, dominated by N-trans-caffeoyltyramine. The profile of oil polar extracts contained hydroxycinnamic acid derivatives and cannabinoids at lower extent. While the extracts from hemp seed and flour did not interfere with growth of Caco-2 and HT-29 cell, the one from oil (150 µg/mL) significantly reduced cell viability after 24 h of treatment. This effect was associated with the activation of apoptotic cell death and was independent from the antioxidant capacity of the oil polar extract. Notably, HT-29 cells differentiated with sodium butyrate were not sensitive to the cytotoxic effect of the oil extract.”
https://www.ncbi.nlm.nih.gov/pubmed/31544542
https://www.tandfonline.com/doi/abs/10.1080/09637486.2019.1666804?journalCode=iijf20
Perception of Benefits and Harms of Medical Cannabis among Seriously Ill Patients in an Outpatient Palliative Care Practice.

“Patients with serious illness often have pain, uncontrolled symptoms, and poor quality of life. Evidence continues to evolve regarding the role of cannabis to treat chronic pain, nausea, and anorexia. Little is known about how patients with serious illness perceive its benefits and harms. Given that an increasing number of clinicians across the United States are treating patients with medical cannabis, it is important for providers to understand patient beliefs about this modality. We assessed patient perceptions of benefits and harms of cannabis who obtained a medical cannabis card within an ambulatory palliative care (APC) practice.
Results: All 101 patients invited to participate completed the survey. A majority had cancer (76%) and were married (61%), disabled or retired (75%), older than 50 years of age (64%), and men (56%). Most patients ingested (61%) or vaporized (49%) cannabis products. A majority of respondents perceived cannabis to be important for their pain (96%) management. They reported that side effects were minimally bothersome, and drowsiness was the most commonly reported bothersome harm (28%). A minority of patients reported cannabis withdrawal symptoms (19%) and concerns for dependency (14%). The majority of patients were using concurrent prescription opioids (65%). Furthermore, a majority of cancer patients reported cannabis as being important for cancer cure (59%).
Conclusion: Patients living with serious illnesses who use cannabis in the context of a multidisciplinary APC practice use cannabis for curative intent and for pain and symptom control. Patients reported improved pain, other symptoms, and a sense of well-being with few reported harms.”
Evaluation of the effects of cannabinoids CBD and CBG on human ovarian cancer cells in vitro
 “Ovarian cancer, with over a 90% reoccurrence within 18 months of treatment, and approximately a 30% mortality rate after 5 years, is the leading cause of death in cases of gynaecological malignancies. Acquired resistance, and toxic side effects by clinically used agents are major challenges associated with current treatments, indicating the need for new approaches in ovarian cancer treatment.
“Ovarian cancer, with over a 90% reoccurrence within 18 months of treatment, and approximately a 30% mortality rate after 5 years, is the leading cause of death in cases of gynaecological malignancies. Acquired resistance, and toxic side effects by clinically used agents are major challenges associated with current treatments, indicating the need for new approaches in ovarian cancer treatment.
Increased tumour cell proliferation associated with upregulation of cannabinoid (CB) receptors has been observed in ovarian cancer. As cannabinoids reported to bind to CB receptors, and can potentially modulate their downstream signalling, this raises the possibility of cannabinoids as potential anticancer drugs for ovarian cancer treatment.
Amongst the cannabinoids, non-psychoactive CBD and CBG have been shown to have anticancer activities towards prostate and colon cancer cells through multiple mechanisms of action. However, CBD and CBG have yet to be investigated in relation to ovarian cancer therapy either in vitro or in vivo.
Aim:
The aims of this study were to evaluate the potential cytotoxic effects of CBD and CBG in human ovarian cancer cells, their ability to potentiate existing clinically used agents for ovarian cancer, and to perform initial mode of action studies in vitro.
Conclusions:
Both CBD and CBG showed preferential cytotoxicity against the ovarian cancer cells analysed compared to the non-cancer cells; however, this was less than for carboplatin. Importantly, in contrast to carboplatin, CBD and CBG showed similar activity towards cisplatin sensitive and cisplatin resistant cells indicating distinctive mechanisms of action to platinum drugs.
Preferential cytotoxicity towards cancer cells in vitro and ability to potentiate carboplatin and overcome cisplatin resistance identify CBD and CBG as promising candidates that warrant further investigation, both in terms of detailed mechanism of action studies and also in vivo studies to assess whether this promising activity translates into an in vivo setting and their potential for further progression towards the clinic.”