
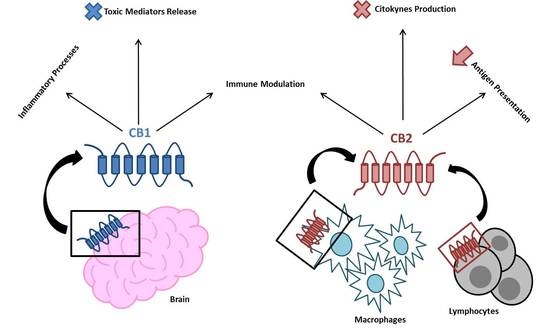
![]() “Endocannabinoid system consists of cannabinoid type 1 (CB1) and cannabinoid type 2 (CB2) receptors, their endogenous ligands, and the enzymes responsible for their synthesis and degradation. CB2, to a great extent, and CB1, to a lesser extent, are involved in regulating the immune response. They also regulate the inflammatory processes by inhibiting pro-inflammatory mediator release and immune cell proliferation. This review provides an overview on the role of the endocannabinoid system with a major focus on cannabinoid receptors in the pathogenesis and onset of inflammatory and autoimmune pediatric diseases, such as immune thrombocytopenia, juvenile idiopathic arthritis, inflammatory bowel disease, celiac disease, obesity, neuroinflammatory diseases, and type 1 diabetes mellitus. These disorders have a high social impact and represent a burden for the healthcare system, hence the importance of individuating more innovative and effective treatments. The endocannabinoid system could address this need, representing a possible new diagnostic marker and therapeutic target.”
“Endocannabinoid system consists of cannabinoid type 1 (CB1) and cannabinoid type 2 (CB2) receptors, their endogenous ligands, and the enzymes responsible for their synthesis and degradation. CB2, to a great extent, and CB1, to a lesser extent, are involved in regulating the immune response. They also regulate the inflammatory processes by inhibiting pro-inflammatory mediator release and immune cell proliferation. This review provides an overview on the role of the endocannabinoid system with a major focus on cannabinoid receptors in the pathogenesis and onset of inflammatory and autoimmune pediatric diseases, such as immune thrombocytopenia, juvenile idiopathic arthritis, inflammatory bowel disease, celiac disease, obesity, neuroinflammatory diseases, and type 1 diabetes mellitus. These disorders have a high social impact and represent a burden for the healthcare system, hence the importance of individuating more innovative and effective treatments. The endocannabinoid system could address this need, representing a possible new diagnostic marker and therapeutic target.”
https://www.ncbi.nlm.nih.gov/pubmed/31771129
https://www.mdpi.com/1422-0067/20/23/5875





 “The cannabinoid (CB) receptor 2, primarily expressed in immune cells, was shown to play important immune-regulatory functions. In particular, the CB2-R63 functional variant has been shown to alter the ability of the CB2 receptor to exert its inhibitory function on T lymphocytes.
The aim of this study was to investigate the association between a common dinucleotide polymorphism, Q63R, in the cannabinoid receptor 2 gene (CNR2) and rheumatoid arthritis (RA) in the Lebanese population.
One hundred five unrelated Lebanese RA patients and one hundred five controls from different Lebanese governorates were recruited in this study. Genomic DNA was extracted, polymerase chain reaction was performed, and CNR2 was genotyped in a blinded fashion. The χ2 test was used to determine the differences in genotypes and allele frequencies. CNR2 genotyping showed significantly higher frequencies of the CB2-R63 variant (allele frequencies, P < 0.00001; genotype distribution, P < 0.00001) in RA patients when compared with healthy controls. Moreover, RR carriers had more than 10-fold risk for developing RA (OR = 10.8444, 95% CI = 5.0950-23.0818; P < 0.0001), and QR carriers had more than 3-fold risk (OR = 3.8667, 95% CI = 1.7886-8.3591; P = 0.0006) as compared with QQ carriers.
Our preliminary results suggest a role of CB2-Q63R gene polymorphism in the etiology of RA, thus supporting its potential use as a pharmacological target for selective agonists in clinical practice.”
“The cannabinoid (CB) receptor 2, primarily expressed in immune cells, was shown to play important immune-regulatory functions. In particular, the CB2-R63 functional variant has been shown to alter the ability of the CB2 receptor to exert its inhibitory function on T lymphocytes.
The aim of this study was to investigate the association between a common dinucleotide polymorphism, Q63R, in the cannabinoid receptor 2 gene (CNR2) and rheumatoid arthritis (RA) in the Lebanese population.
One hundred five unrelated Lebanese RA patients and one hundred five controls from different Lebanese governorates were recruited in this study. Genomic DNA was extracted, polymerase chain reaction was performed, and CNR2 was genotyped in a blinded fashion. The χ2 test was used to determine the differences in genotypes and allele frequencies. CNR2 genotyping showed significantly higher frequencies of the CB2-R63 variant (allele frequencies, P < 0.00001; genotype distribution, P < 0.00001) in RA patients when compared with healthy controls. Moreover, RR carriers had more than 10-fold risk for developing RA (OR = 10.8444, 95% CI = 5.0950-23.0818; P < 0.0001), and QR carriers had more than 3-fold risk (OR = 3.8667, 95% CI = 1.7886-8.3591; P = 0.0006) as compared with QQ carriers.
Our preliminary results suggest a role of CB2-Q63R gene polymorphism in the etiology of RA, thus supporting its potential use as a pharmacological target for selective agonists in clinical practice.”