
 “Objectives: This article presents findings from a large prospective examination of Canadian medical cannabis patients, with a focus on the impacts of cannabis on prescription opioid use and quality of life over a 6-month period.
“Objectives: This article presents findings from a large prospective examination of Canadian medical cannabis patients, with a focus on the impacts of cannabis on prescription opioid use and quality of life over a 6-month period.
Results: Participants were 57.6% female, with a median age of 52 years. Baseline opioid use was reported by 28% of participants, dropping to 11% at 6 months. Daily opioid use went from 152 mg morphine milligram equivalent (MME) at baseline to 32.2 mg MME at 6 months, a 78% reduction in mean opioid dosage. Similar reductions were also seen in the other four primary prescription drug classes identified by participants, and statistically significant improvements were reported in all four domains of the WHOQOL-BREF.
Conclusions: This study provides an individual-level perspective of cannabis substitution for opioids and other prescription drugs, as well as associated improvement in quality of life over 6 months. The high rate of cannabis use for chronic pain and the subsequent reductions in opioid use suggest that cannabis may play a harm reduction role in the opioid overdose crisis, potentially improving the quality of life of patients and overall public health.”
https://pubmed.ncbi.nlm.nih.gov/33367882/
![]()
 “Chronic pelvic pain (CPP) affects up to 15% of women in the United States. The endocannabinoid system is a potential pharmacological target for pelvic pain as cannabinoid receptors are highly expressed in the uterus and other nonreproductive tissues.
“Chronic pelvic pain (CPP) affects up to 15% of women in the United States. The endocannabinoid system is a potential pharmacological target for pelvic pain as cannabinoid receptors are highly expressed in the uterus and other nonreproductive tissues. “Opioid misuse and overuse has contributed to a widespread overdose crisis and many patients and physicians are considering medical cannabis to support opioid tapering and chronic pain control. Using a five-step modified Delphi process, we aimed to develop consensus-based recommendations on: 1) when and how to safely initiate and titrate cannabinoids in the presence of opioids, 2) when and how to safely taper opioids in the presence of cannabinoids, and 3) how to monitor patients and evaluate outcomes when treating with opioids and cannabinoids.
“Opioid misuse and overuse has contributed to a widespread overdose crisis and many patients and physicians are considering medical cannabis to support opioid tapering and chronic pain control. Using a five-step modified Delphi process, we aimed to develop consensus-based recommendations on: 1) when and how to safely initiate and titrate cannabinoids in the presence of opioids, 2) when and how to safely taper opioids in the presence of cannabinoids, and 3) how to monitor patients and evaluate outcomes when treating with opioids and cannabinoids. “Chronic pelvic pain affects women across all demographics. Its management is complex and requires a multimodal approach.
“Chronic pelvic pain affects women across all demographics. Its management is complex and requires a multimodal approach. “The prevalence of cancer pain will continue to rise as pain is common among the survivorship and general cancer population. As interest in cannabis and cannabinoids for medicinal use including pain management continues to rise, there is growing need to update and review the current state of evidence for their use. The literature was searched for articles in English with key words cannabis, cannabinoids, and cancer pain. The sources of articles were PubMed, Embase, and open Google search.
“The prevalence of cancer pain will continue to rise as pain is common among the survivorship and general cancer population. As interest in cannabis and cannabinoids for medicinal use including pain management continues to rise, there is growing need to update and review the current state of evidence for their use. The literature was searched for articles in English with key words cannabis, cannabinoids, and cancer pain. The sources of articles were PubMed, Embase, and open Google search. “Although studied in a few randomized controlled trials (RCTs), the efficacy of medical cannabis (MC) for chronic pain remains controversial. Using an alternative approach, this multicenter, questionnaire-based prospective cohort was aimed to assess the long-term effects of MC on chronic pain of various etiologies and to identify predictors for MC treatment success.
“Although studied in a few randomized controlled trials (RCTs), the efficacy of medical cannabis (MC) for chronic pain remains controversial. Using an alternative approach, this multicenter, questionnaire-based prospective cohort was aimed to assess the long-term effects of MC on chronic pain of various etiologies and to identify predictors for MC treatment success.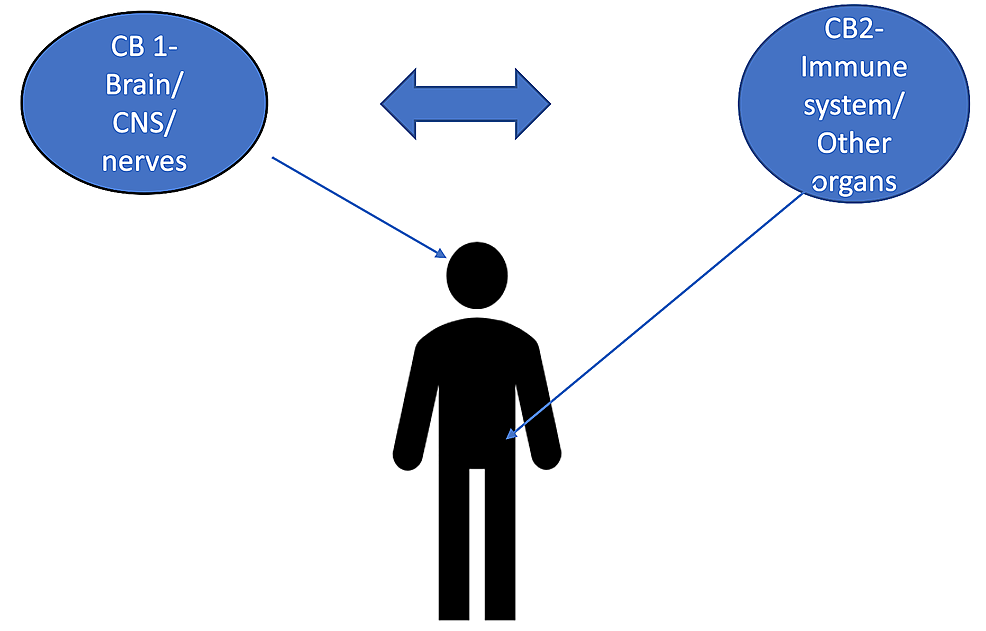 “The burden of chronic pain has affected many individuals leading to distress and discomfort, alongside numerous side effects with conventional therapeutic approaches.
“The burden of chronic pain has affected many individuals leading to distress and discomfort, alongside numerous side effects with conventional therapeutic approaches. “Cannabinoids help in pain treatment through their action on CB1 and CB2 receptors.
“Cannabinoids help in pain treatment through their action on CB1 and CB2 receptors.