“We conducted a systematic review to determine the efficacy and safety of cannabidiol (CBD) for chronic pain.
CBD and tetrahydrocannabinol (THC), both from Cannabis plants with almost identical chemical structures, attach to the CB receptor, eliciting different effects like the psychoactivity seen on THC but less or none in CBD.
Regulations of CBD worldwide differ from each other due to the insufficiency of solid evidence to establish its benefit versus the risks. However, a few studies are showing the benefits of CBD not only for chronic pain but also for sleep improvement and quality of life.
In conclusion, CBD is an excellent alternative to an opioid in chronic pain because CBD is non-intoxicating in its pure form. More clinical trials should be done to prove CBD’s significance clinically and statistically.”
“It is essential to know that pure CBD extract is a strong candidate as an alternative to opioid medication since it is nonintoxicating and dependence is less. This systematic review can benefit other researchers and even ordinary people eager to know the latest updates on CBD research on chronic pain. In the future, clinical trials should focus more on using pure CBD extract to treat chronic pain to attain evidence to properly recommend CBD in the health insurance sector so that patients may benefit to the full extent.”
“Cannabinoid-based therapies offer a safer, non-opioid alternative for the management of chronic pain. While most studies focus on the analgesic potential of the main psychoactive component of marijuana, Δ9-tetrahydrocannabinol, fewer studies have investigated the role of the non-psychoactive component, cannabidiol (CBD). CBD has been purported to have analgesic, anti-inflammatory, anticonvulsant, and anxiolytic effects. In addition to having actions at both cannabinoid receptors (CB1 and CB2 ), CBD has been shown to interact with both the transient receptor potential vanilloid-1 (TRPV1) and serotonergic (5-HT) receptors. Clinically, CBD’s lack of psychoactivity and decreased abuse liability make it an appealing pharmacotherapeutic for the management of chronic pain. Therefore, the purpose of the current study was to determine whether CBD sex- or dose-dependently reverses antinociception in an acute model of thermal pain and/or mechanical allodynia in a model of cisplatin-induced chronic neuropathic pain. Furthermore, we observed the degree to which CB1 , CB2 , 5-HT, and TRPV1 receptors may be mediating these anti-allodynic responses. Male and female wild-type mice were assessed for either the anti-allodynic effects of 0, 1, 3, 10, and 30 mg/kg CBD in a cisplatin-induced model of neuropathic pain or the antinociceptive effects of 0, 1, 3, 10, 30, and 100 mg/kg CBD in a model of acute thermal (tail-flick) pain 60 minutes following CBD administration. To determine the relative contributions of each receptor subtype in mediating the anti-allodynic effects of CBD, male and female mice were pretreated with either: vehicle, the CB1 inverse agonist SR141716A (10 mg/kg), the CB2 antagonist SR144528 (10 mg/kg), the TRPV1 antagonist capsazepine (10 mg/kg), or the 5-HT2 antagonist methysergide (4 mg/kg) 30 minutes prior to treatment with CBD. Mice were assessed for the effects of the pretreatment alone and in combination with CBD. CBD at a dose of 3 mg/kg was able to partially reverse cisplatin-induced allodynia in male and female mice, while doses of 10 and 30 mg/kg resulted in nearly complete reversal. Our preliminary findings showed that the anti-allodynic effects of 30 mg/kg CBD were completely blocked following pretreatment with SR141716A and SR144528, and partially blocked by capsazepine in both male and female mice. Interestingly, pretreatment with methysergide partially attenuated the anti-allodynic effects of CBD in females alone. In contrast, CBD (0-100 mg/kg) failed to induce antinociception on the tail-flick assay. CBD did induce mild hypothermia with males showing a greater degree of CBD-mediated hypothermia than female mice. Taken together, these findings suggest that CBD may be a more effective treatment option for the management of chronic pain. This study highlights the therapeutic potential of CBD in a model of neuropathic pain and suggests that these effects may have clinical implications for the use of cannabinoids in chronic pain management.”
“Despite the importance of pain as a warning physiological system, chronic neuropathic pain is frequently caused by damage in the nervous system, followed by persistence over a long period, even in the absence of dangerous stimuli or after healing of injuries. Chronic neuropathic pain affects hundreds of millions of adults worldwide, creating a direct impact on quality of life. This pathology has been extensively characterized concerning its cellular and molecular mechanisms, and the endocannabinoid system (eCS) is widely recognized as pivotal in the development of chronic neuropathic pain. Scientific evidence has supported that phyto-, synthetic and endocannabinoids are efficient for pain management, while strong data arise from the therapeutic use of Cannabis-derived products. The use of medicinal Cannabis products is directed toward not only relieving symptoms of chronic pain, but also improving several aspects of patients’ welfare. Here, we review the involvement of eCS, along with other cellular and molecular elements, in chronic neuropathic pain pathology and how this system can be targeted for pain management.”
“The role of eCS as a pharmacological target and the advantages of using medicinal Cannabis sp. to treat pain is remarkable, as described in this review.”
“Background: Neuropathic symptoms have a wide variety of manifestations, ranging from pain to pruritus. Neuropathic pruritus is a type of chronic pruritus related to damaged small fibers. Cannabinoids have evidence to manage neuropathic symptoms. We present a case of refractory neuropathic pruritus that was successfully managed with the use of oral cannabinoids.
Case presentation: A 60-year-old male with amyotrophic lateral sclerosis with ongoing pruritus despite the use of standard neuropathic therapies.
Formulation of a plan: A balanced oral cannabinoid from a licensed producer was preferred as it has evidence for neuropathic symptoms and is generally well tolerated.
Outcome: The patient showed improvement to his pruritus score from 7/10 to 3/10. There was initial increased sedation but tolerance developed quickly.
Lessons learned from case: Cannabinoids are possibly safe and effective in management of neuropathic pruritus.”
“Neuropathic pruritus is a chronic form of pruritus that causes significant symptom burden and can be difficult to treat. Cannabinoids have evidence to manage chronic neuropathic pain. This case demonstrates the safe and effective use of cannabinoids to manage neuropathic pruritus.”
“Cannabinoid-based medications possess unique multimodal analgesic mechanisms of action, modulating diverse pain targets.
Cannabinoids are classified based on their origin into three categories: endocannabinoids (present endogenously in human tissues), phytocannabinoids (plant derived) and synthetic cannabinoids (pharmaceutical). Cannabinoids exert an analgesic effect, peculiarly in hyperalgesia, neuropathic pain and inflammatory states.
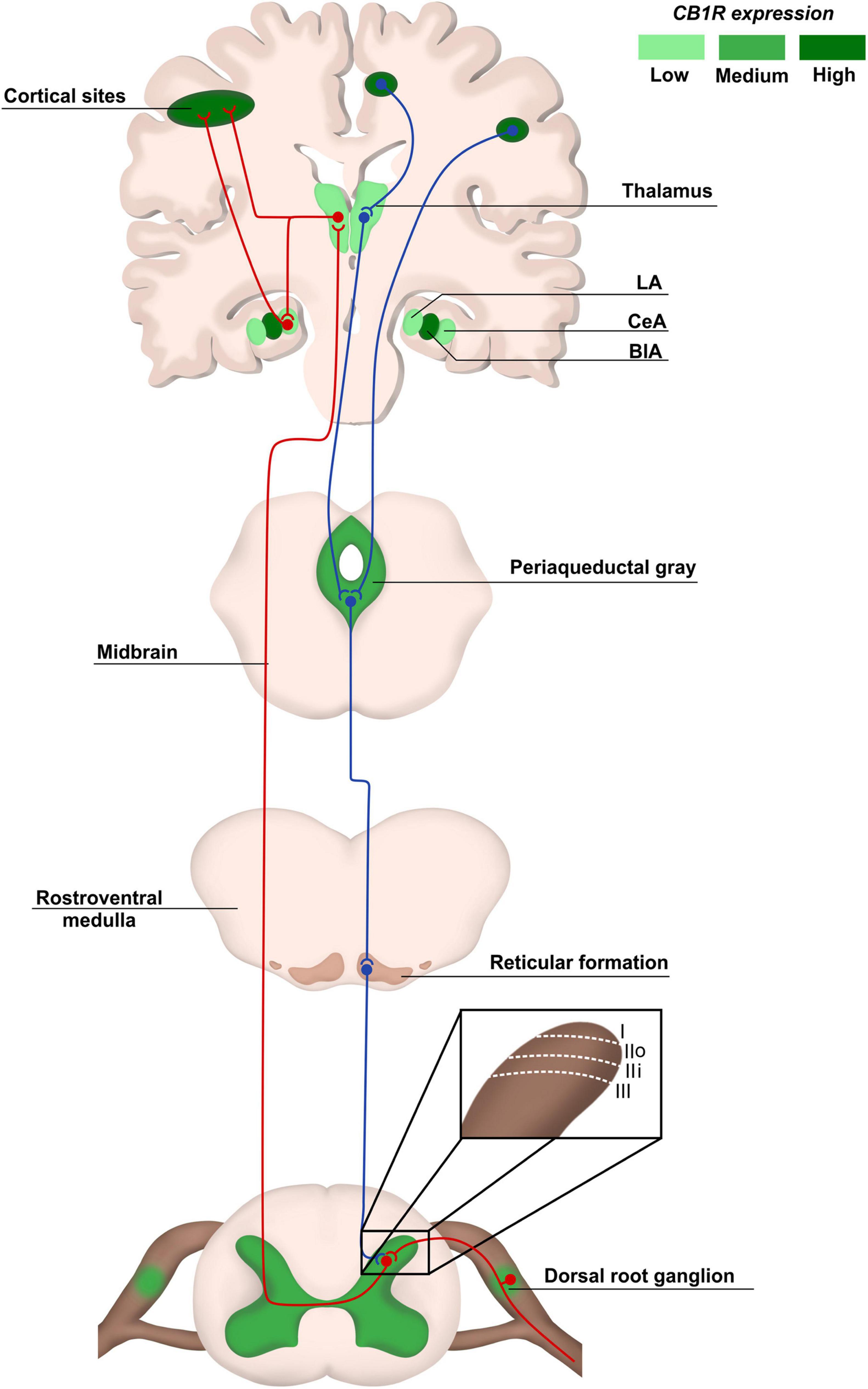
Endocannabinoids are released on demand from postsynaptic terminals and travels retrograde to stimulate cannabinoids receptors on presynaptic terminals, inhibiting the release of excitatory neurotransmitters. Cannabinoids (endogenous and phytocannabinoids) produce analgesia by interacting with cannabinoids receptors type 1 and 2 (CB1 and CB2), as well as putative non-CB1/CB2 receptors; G protein-coupled receptor 55, and transient receptor potential vanilloid type-1. Moreover, they modulate multiple peripheral, spinal and supraspinal nociception pathways.
Cannabinoids-opioids cross-modulation and synergy contribute significantly to tolerance and antinociceptive effects of cannabinoids. This narrative review evaluates cannabinoids’ diverse mechanisms of action as it pertains to nociception modulation relevant to the practice of anesthesiologists and pain medicine physicians.”
“Many people with MS (pwMS) use unregulated cannabis or cannabis products to treat the symptoms associated with the disease. In line with this, Sativex, a synthetic combination of cannabidiol (CBD) and Δ9-tetrahydrocannabinol (Δ9-THC) has been approved to treat symptoms of spasticity.
In animals, CBD is effective in reducing the amounts of T-cell infiltrates in the spinal cord, suggesting CBD has anti-inflammatory properties. By doing this, CBD has shown to delay symptom onset in animal models of multiple sclerosis and slow disease progression. Importantly, combinations of CBD and Δ9-THC appear more effective in treating animal models of multiple sclerosis.
While CBD reduces the amounts of cell infiltrates in the spinal cord, Δ9-THC reduces scores of spasticity. In human studies, the results are less encouraging and conflict with the findings in animals. Drugs which deliver a combination of Δ9-THC and CBD in a 1:1 ratio appear to be only moderately effective in reducing spasticity scores, but appear to be almost as effective as current front-line treatments and cause less severe side effects than other treatments, such as baclofen (a GABA-B receptor agonist) and tizanidine (an α2 adrenergic receptor agonist).
The findings of the studies reviewed suggest that cannabinoids may help treat neuropathic pain in pwMS as an add-on therapy to already established pain treatments.
Long term double-blind placebo studies are greatly needed to further our understanding of the role of cannabinoids in multiple sclerosis treatment.”
“Recent studies have shown that cannabidiol (CBD) could have a great therapeutic potential for treating disorders such as chronic pain and anxiety. In the target article, the authors propose that CBD modulates serotonergic transmission and reverses allodynia and anxiety-like behaviour in a rat model of neuropathic pain. Furthermore, this study shows an antinociceptive effect mediated by TRPV1 and partially by 5-HT1A receptors, as well as an anxiolytic effect mediated by 5-HT1A receptors.”
“Cannabidiol modulates serotonergic transmission and reverses both allodynia and anxiety-like behavior in a model of neuropathic pain” https://pubmed.ncbi.nlm.nih.gov/30157131/
“Diabetes is a chronic disease associated with a high number of complications such as peripheral neuropathy, which causes sensorial disturbances and may lead to the development of diabetic neuropathic pain (DNP). The current treatment for DNP is just palliative and the drugs may cause severe adverse effects, leading to discontinuation of treatment. Thus, new therapeutic targets need to be urgently investigated.
Studies have shown that cannabinoids have promising effects in the treatment of several pathological conditions, including chronic pain.
Thus, we aimed to investigate the acute effect of the intrathecal injection of CB1 or CB2 cannabinoid receptor agonists N-(2-chloroethyl)-5Z, 8Z, 11Z, 14Z-eicosatetraenamide (ACEA) or JWH 133, respectively (10, 30 or 100 μg/rat) on the mechanical allodynia associated with experimental diabetes induced by streptozotocin (60 mg/kg; intraperitoneal) in rats.
Cannabinoid receptor antagonists CB1 AM251 or CB2 AM630 (1 mg/kg) were given before treatment with respective agonists to confirm the involvement of cannabinoid CB1 or CB2 receptors. Rats with diabetes exhibited a significant reduction on the paw mechanical threshold 2 weeks after diabetes induction, having the maximum effect observed 4 weeks after the streptozotocin injection. This mechanical allodynia was significantly improved by intrathecal treatment with ACEA or JWH 133 (only at the higher dose of 100 μg). Pre-treatment with AM251 or AM630 significantly reverted the anti-allodynic effect of the ACEA or JWH 133, respectively.
Considering the clinical challenge that the treatment of DPN represents, this study showed for the first time, that the intrathecal cannabinoid receptors agonists may represent an alternative for the treatment of DNP.”
“Cannabinoid CB2 receptor (CB2) agonists are potential analgesics void of psychotropic effects.
Peripheral immune cells, neurons and glia express CB2, however the involvement of CB2 from these cells in neuropathic pain remains unresolved. We explored spontaneous neuropathic pain through on-demand self-administration of the selective CB2 agonist JWH133 in wild-type and knockout mice lacking CB2 in neurons, monocytes or constitutively. Operant self-administration reflected drug-taking to alleviate spontaneous pain, nociceptive and affective manifestations. While constitutive deletion of CB2 disrupted JWH133-taking behavior, this behavior was not modified in monocyte-specific CB2 knockouts and was increased in mice defective in neuronal CB2 knockouts suggestive of increased spontaneous pain. Interestingly, CB2-positive lymphocytes infiltrated the injured nerve and possible CB2transfer from immune cells to neurons was found. Lymphocyte CB2depletion also exacerbated JWH133 self-administration and inhibited antinociception.
This work identifies a simultaneous activity of neuronal and lymphoid CB2that protects against spontaneous and evoked neuropathic pain.”


 “Human immunodeficiency virus (HIV) infection and antiretroviral therapy can independently induce HIV-associated neuropathic pain (HIV-NP).
“Human immunodeficiency virus (HIV) infection and antiretroviral therapy can independently induce HIV-associated neuropathic pain (HIV-NP).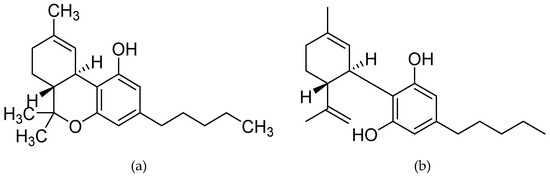
 “Recent studies have shown that cannabidiol (CBD) could have a great therapeutic potential for treating disorders such as chronic pain and anxiety. In the target article, the authors propose that CBD modulates serotonergic transmission and reverses allodynia and anxiety-like behaviour in a rat model of neuropathic pain. Furthermore, this study shows an antinociceptive effect mediated by TRPV1 and partially by 5-HT1A receptors, as well as an anxiolytic effect mediated by 5-HT1A receptors.”
“Recent studies have shown that cannabidiol (CBD) could have a great therapeutic potential for treating disorders such as chronic pain and anxiety. In the target article, the authors propose that CBD modulates serotonergic transmission and reverses allodynia and anxiety-like behaviour in a rat model of neuropathic pain. Furthermore, this study shows an antinociceptive effect mediated by TRPV1 and partially by 5-HT1A receptors, as well as an anxiolytic effect mediated by 5-HT1A receptors.” “Diabetes is a chronic disease associated with a high number of complications such as peripheral neuropathy, which causes sensorial disturbances and may lead to the development of diabetic neuropathic pain (DNP). The current treatment for DNP is just palliative and the drugs may cause severe adverse effects, leading to discontinuation of treatment. Thus, new therapeutic targets need to be urgently investigated.
“Diabetes is a chronic disease associated with a high number of complications such as peripheral neuropathy, which causes sensorial disturbances and may lead to the development of diabetic neuropathic pain (DNP). The current treatment for DNP is just palliative and the drugs may cause severe adverse effects, leading to discontinuation of treatment. Thus, new therapeutic targets need to be urgently investigated.