“Pain is a common and complex symptom of cancer having physical, social, spiritual and psychological aspects. Approximately 70%-80% of cancer patients experiences pain, as reported in India.
“Pain is a common and complex symptom of cancer having physical, social, spiritual and psychological aspects. Approximately 70%-80% of cancer patients experiences pain, as reported in India.
Ayurveda recommends use of Shodhita (Processed) Bhanga (Cannabis) for the management of pain but no research yet carried out on its clinical effectiveness.
OBJECTIVE:
To assess the analgesic potential of Jala-Prakshalana (Water-wash) processed Cannabis sativa L. leaves powder in cancer patients with deprived quality of life (QOL) through openlabel single arm clinical trial.
MATERIALS AND METHODS:
Waterwash processed Cannabis leaves powder filled in capsule, was administered in 24 cancer patients with deprived QOL presenting complaints of pain, anxiety or depression; for a period of 4 weeks; in a dose of 250 mg thrice a day; along with 50 ml of cow’s milk and 4 g of crystal sugar. Primary outcome i.e. pain was measured by Wong-Bakers FACES Pain Scale (FACES), Objective Pain Assessment (OPA) scale and Neuropathic Pain Scale (NPS). Secondary outcome namely anxiety was quantified by Hospital Anxiety and Depression Scale (HADS), QOL by FACT-G scale, performance score by Eastern Cooperative Oncology Group (ECOG) and Karnofsky score.
RESULTS:
Significant reduction in pain was found on FACES Pain Scale (P < 0.05), OPA (P < 0.05), NPS (P < 0.001), HADS (P < 0.001), FACT-G scale (P < 0.001), performance status score like ECOG (P < 0.05) and Karnofsky score (P < 0.01).
CONCLUSION:
Jalaprakshalana Shodhita Bhanga powder in a dose of 250 mg thrice per day; relieves cancer induced pain, anxiety and depression significantly and does not cause any major adverse effect and withdrawal symptoms during trial period.”
 “Despite improvements in medical care, patients with advanced cancer still experience substantial symptom distress. There is increasing interest in the use of medicinal
“Despite improvements in medical care, patients with advanced cancer still experience substantial symptom distress. There is increasing interest in the use of medicinal  “Cannabidiol (CBD) has emerged as a potential agent for breast cancer management.
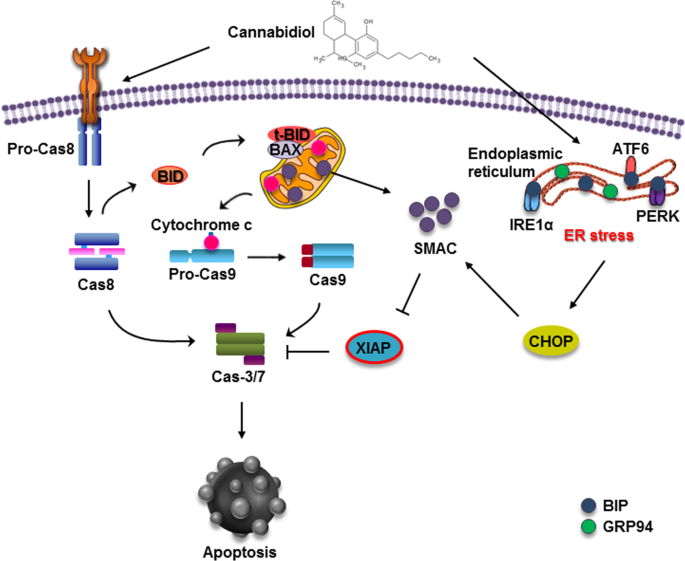
“Cannabidiol (CBD) has emerged as a potential agent for breast cancer management.
 “There is considerable interest in the use of cannabinoids for symptom control in palliative care, but there is little high-quality evidence to guide clinical practice.
“There is considerable interest in the use of cannabinoids for symptom control in palliative care, but there is little high-quality evidence to guide clinical practice. “A 64 year old male heating engineer was investigated for a persistent cough and found to have epithelioid mesothelioma with pleural effusion, lung nodules and increased thoracic lymph nodes. He declined standard of care treatment following his own research and he was enrolled in a named patient programme of IMM-101. He was advised to correct his low vitamin D3 level and to start using anti-inflammatories such as aspirin, bromelain and low dose Naltrexone. At review one year later a CT scan showed no change and he continued on the regimen. Four years after the diagnosis a CT scan showed that there was a modest but definite progression of the left malignant pleural thickening, and a new right-sided effusion, enlargement of several intrathoracic nodes which had been noted on the early scans. The chest wall lump eventually broke down and required local radiotherapy. He then developed abdominal pain and found to have peritoneal disease. Last year he obtained the
“A 64 year old male heating engineer was investigated for a persistent cough and found to have epithelioid mesothelioma with pleural effusion, lung nodules and increased thoracic lymph nodes. He declined standard of care treatment following his own research and he was enrolled in a named patient programme of IMM-101. He was advised to correct his low vitamin D3 level and to start using anti-inflammatories such as aspirin, bromelain and low dose Naltrexone. At review one year later a CT scan showed no change and he continued on the regimen. Four years after the diagnosis a CT scan showed that there was a modest but definite progression of the left malignant pleural thickening, and a new right-sided effusion, enlargement of several intrathoracic nodes which had been noted on the early scans. The chest wall lump eventually broke down and required local radiotherapy. He then developed abdominal pain and found to have peritoneal disease. Last year he obtained the  “The purpose of this study is to gain a greater understanding of cancer survivors’ attitudes, perspectives, and concerns about medical cannabinoids (MCs) for cancer symptom and side effect management.
“The purpose of this study is to gain a greater understanding of cancer survivors’ attitudes, perspectives, and concerns about medical cannabinoids (MCs) for cancer symptom and side effect management.
 “The monocyclic 1,4-benzoquinone, HU-331, the direct oxidation product of
“The monocyclic 1,4-benzoquinone, HU-331, the direct oxidation product of  “According to recent studies,
“According to recent studies,