 “Industrial hemp is a multiuse crop that has been widely cultivated to produce fibers and nutrients. The capability of the essential oil (EO) from inflorescences as antimicrobial agent has been reported. However, literature data are still lacking about the hemp EO antiprotozoal efficacy in vivo.
“Industrial hemp is a multiuse crop that has been widely cultivated to produce fibers and nutrients. The capability of the essential oil (EO) from inflorescences as antimicrobial agent has been reported. However, literature data are still lacking about the hemp EO antiprotozoal efficacy in vivo.
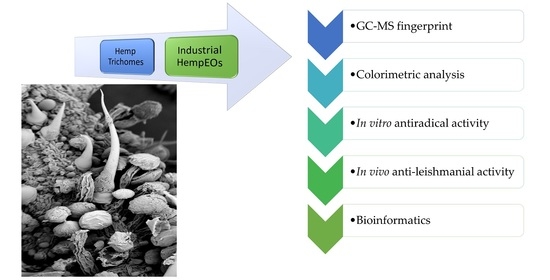
The present study aims to unravel this concern through the evaluation of the efficacy of hemp EOs (2.5 mL/kg, intraperitoneally) of three different cultivars, namely Futura 75, Carmagnola selezionata and Eletta campana, in mice intraperitoneally infected with Leishmania tropica. A detailed description of EO composition and targets-components analysis is reported.
Myrcene, α-pinene and E-caryophyllene were the main components of the EOs, as indicated by the gas-chromatographic analysis. However, a prominent position in the scenario of the theoretical interactions underlying the bio-pharmacological activity was also occupied by selina-3,7(11)-diene, which displayed affinities in the micromolar range (5.4-28.9) towards proliferator-activated receptor α, cannabinoid CB2 receptor and acetylcholinesterase. The content of this compound was higher in Futura 75 and Eletta campana, in accordance with their higher scavenging/reducing properties and efficacy against the tissue wound, induced by L. tropica.
Overall, the present study recommends hemp female inflorescences, as sources of biomolecules with potential pharmacological applications, especially towards infective diseases.”
https://pubmed.ncbi.nlm.nih.gov/33673274/
https://www.mdpi.com/2218-273X/11/2/272

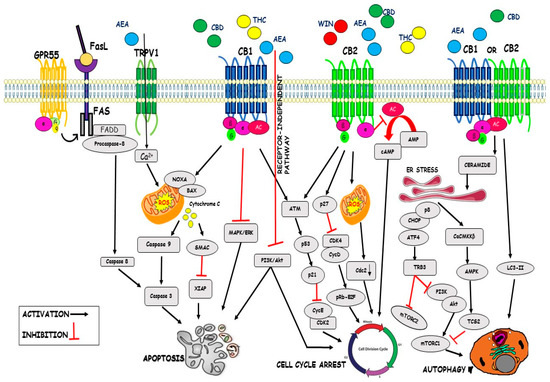
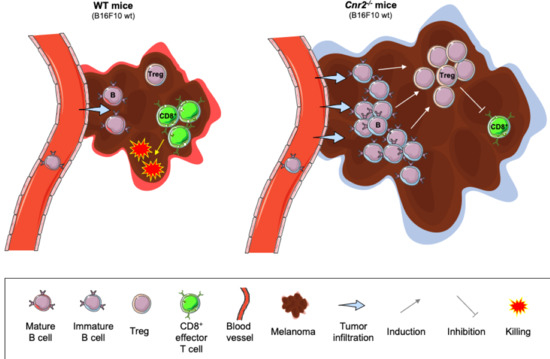
 “Colorectal cancer (CRC) is between the top three occurring cancers worldwide. The anticancer effects of Cannabinoid receptor 2 (CB
“Colorectal cancer (CRC) is between the top three occurring cancers worldwide. The anticancer effects of Cannabinoid receptor 2 (CB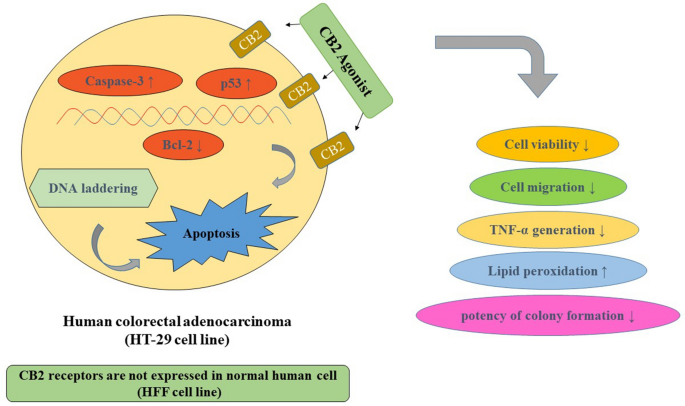
 “
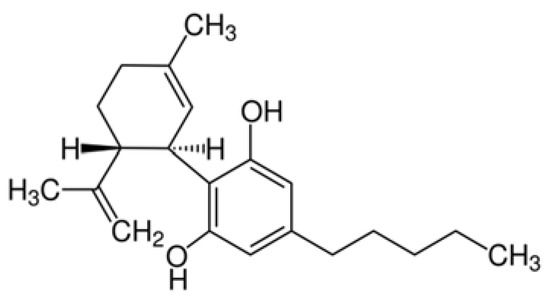
“ “We previously reported that cannabidiol (CBD), a cannabinoid with a low toxicity profile, downregulated the expression of the prometastatic gene inhibitor of DNA binding 1 (
“We previously reported that cannabidiol (CBD), a cannabinoid with a low toxicity profile, downregulated the expression of the prometastatic gene inhibitor of DNA binding 1 ( “The transcription factor NFκB drives neoplastic progression of many cancers including primary brain tumors (glioblastoma; GBM). Precise therapeutic modulation of NFκB activity can suppress central oncogenic signalling pathways in GBM, but clinically applicable compounds to achieve this goal have remained elusive.
“The transcription factor NFκB drives neoplastic progression of many cancers including primary brain tumors (glioblastoma; GBM). Precise therapeutic modulation of NFκB activity can suppress central oncogenic signalling pathways in GBM, but clinically applicable compounds to achieve this goal have remained elusive.