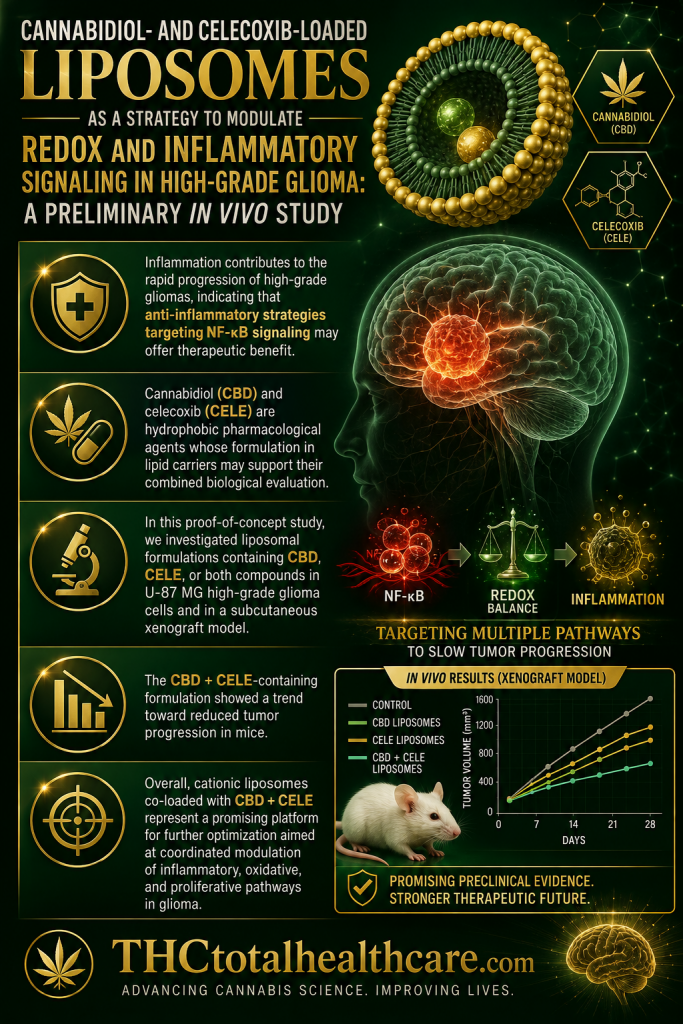
“Inflammation contributes to the rapid progression of high-grade gliomas, indicating that anti-inflammatory strategies targeting NF-κB signaling may offer therapeutic benefit.
Cannabidiol (CBD) and celecoxib (CELE) are hydrophobic pharmacological agents whose formulation in lipid carriers may support their combined biological evaluation.
In this proof-of-concept study, we investigated liposomal formulations containing CBD, CELE, or both compounds in U-87 MG high-grade glioma cells and in a subcutaneous xenograft model.
We assessed cytotoxicity, apoptosis, oxidative stress, Nrf2-dependent responses, NF-κB-centered inflammatory networks, tumor cell invasive properties, and Wnt/β-catenin pathway activity. The nanoformulations induced reactive oxygen species generation by 1.8-fold, which was accompanied by Nrf2 activation. Cationic formulations loaded with the compounds produced more pronounced pro-apoptotic effects (up to 39%) than POPC liposomes, although both types reduced the nuclear translocation of the NF-κB p65 subunit.
The CBD + CELE-containing formulation showed a trend toward reduced tumor progression in mice. It is important to note that the in vitro and in vivo nanoformulations were physicochemically related, but not identical, and the in vivo experiment should be interpreted as a preliminary assessment after intratumoral administration.
Overall, cationic liposomes co-loaded with CBD + CELE represent a promising platform for further optimization aimed at coordinated modulation of inflammatory, oxidative, and proliferative pathways in glioma. However, additional studies, including tissue distribution, release kinetics, and efficacy in orthotopic glioma models, are needed to fully verify their translational potential.”
https://pubmed.ncbi.nlm.nih.gov/42511566
“In summary, this study shows that liposomal formulations containing CBD and CELE, particularly DOTAP:POPC formulations prepared with both compounds, modulate apoptosis, cell cycle distribution, oxidative stress, Nrf2/NF-κB/Wnt-related pathways, and glioma-associated inflammatory mediators in U-87 MG-based models. In the subcutaneous xenograft model, intratumoral administration of the CBD + CELE-containing formulation was associated with a trend toward reduced tumor progression and modulation of selected tumor-associated proteins.”