“Gilles de la Tourette syndrome (GTS) is a neuropsychiatric disorder that is characterized by motor and vocal tics and psychiatric comorbidities, including attention deficit/hyperactivity disorder (ADHD) and obsessive-compulsive behavior/disorder (OCB/OCD). From anecdotal reports and preliminary controlled studies, it is suggested that cannabis-based medicine (CBM) may improve tics and comorbidities in adults with GTS. This study was designed to further investigate efficacy and safety of CBM in GTS and specifically compare effects of different CBM.
“Gilles de la Tourette syndrome (GTS) is a neuropsychiatric disorder that is characterized by motor and vocal tics and psychiatric comorbidities, including attention deficit/hyperactivity disorder (ADHD) and obsessive-compulsive behavior/disorder (OCB/OCD). From anecdotal reports and preliminary controlled studies, it is suggested that cannabis-based medicine (CBM) may improve tics and comorbidities in adults with GTS. This study was designed to further investigate efficacy and safety of CBM in GTS and specifically compare effects of different CBM.
Results: From medical records, we identified 98 patients who had used CBM (most often street cannabis followed by nabiximols, dronabinol, medicinal cannabis) for the treatment of GTS: Of the 38 patients who were able to judge, 66% preferred treatment with medicinal cannabis, 18% dronabinol, 11% nabiximols, and 5% street cannabis. Altogether, CBM resulted in a subjective improvement of tics (of about 60% in 85% of treated cases), comorbidities (55% of treated cases, most often OCB/OCD, ADHD, and sleeping disorders), and quality of life (93%). The effects of CBM appear to persist in the long term. Adverse events occurred in half of the patients, but they were rated as tolerable. Dosages of all CBM varied markedly. Patients assessed cannabis (with a preference for tetrahydrocannabinol [THC]-rich strains) as more effective and better tolerated compared with nabiximols and dronabinol. These data were confirmed by results obtained from the online survey (n=40).
Conclusion: From our results, it is further supported that CBM might be effective and safe in the treatment of tics and comorbidities at least in a subgroup of adult patients with GTS. In our sample, patients favored THC-rich cannabis over dronabinol and nabiximols, which might be related to the entourage effect of cannabis. However, several limitations of the study have to be taken into considerations such as the open uncontrolled design and the retrospective data analysis.”
 “Palliative care is defined by the World Health Organization as “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness…”. The last days and hours of a person’s life can be associated with immense physical as well as emotional suffering Relief of pain and other distressing symptoms, and enhancement of quality of life, are among the essential elements of good palliative care. Palliative care could benefit an estimated 69% to 82% of dying individuals in Canada. As Canada’s population ages, with increasing prevalence of chronic conditions and treatments resulting in prolonged life, it is expected that there will be an increased need for palliative care services.
“Palliative care is defined by the World Health Organization as “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness…”. The last days and hours of a person’s life can be associated with immense physical as well as emotional suffering Relief of pain and other distressing symptoms, and enhancement of quality of life, are among the essential elements of good palliative care. Palliative care could benefit an estimated 69% to 82% of dying individuals in Canada. As Canada’s population ages, with increasing prevalence of chronic conditions and treatments resulting in prolonged life, it is expected that there will be an increased need for palliative care services. “Cannabinoids are pharmacologically active agents extracted from the cannabis plant.
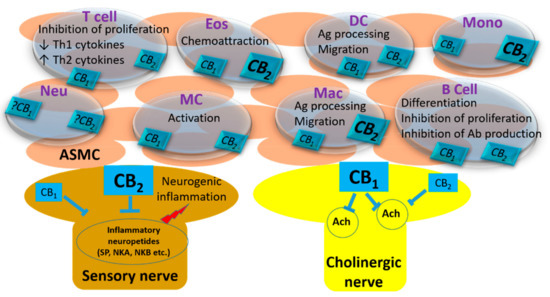
“Cannabinoids are pharmacologically active agents extracted from the cannabis plant.  “The endocannabinoid system (eCB) is a ubiquitous lipid signaling system composed of at least two receptors, their endogenous ligands, and the enzymes responsible for their synthesis and degradation. Within the brain, the eCB system is highly expressed in the hippocampus and controls basic biological processes, including neuronal proliferation, migration and differentiation, which are intimately linked with embryonal neurogenesis. Accumulated preclinical evidence has indicated that eCBs play a major role also in regulating adult neurogenesis. Increased
“The endocannabinoid system (eCB) is a ubiquitous lipid signaling system composed of at least two receptors, their endogenous ligands, and the enzymes responsible for their synthesis and degradation. Within the brain, the eCB system is highly expressed in the hippocampus and controls basic biological processes, including neuronal proliferation, migration and differentiation, which are intimately linked with embryonal neurogenesis. Accumulated preclinical evidence has indicated that eCBs play a major role also in regulating adult neurogenesis. Increased