
“A group of University of Minnesota researchers is testing to see if medical marijuana can help treat chronic pain caused by sickle cell disease, but state and federal laws are putting a hitch in their study.
As researchers continue with the study’s next step — conducting human trials — they’re heading to California, as Minnesota doesn’t easily allow testing cannabis on people. The state’s recently passed medical marijuana law doesn’t include sickle cell disease as a qualifying medical condition, but the University’s current research could play a role in how that law changes in the future.
“We find that cannabinoids have good outcomes in treating pain [in mice with sickle cell disease],” said chief researcher and associate professor of medicine Kalpna Gupta.
Gupta said the researchers are now ready to expand their study to patients. And in doing so, they will move to California, where medical marijuana became legal nearly two decades ago. Minnesota’s stricter version of that law will take effect next summer.
Right now, the Minnesota Department of Health is working to appoint members to a task force that will oversee medical cannabis therapeutic research in the coming months. The department is also fine-tuning the rules that outline patient access and qualifications.
Qualifying health conditions to receive medical cannabis in the Minnesota law include cancer, glaucoma, HIV/AIDS and seizures. Patients also qualify for the drug if they have chronic pain caused by cancer or a terminal illness.
Department of Health spokesman Mike Schommer said symptoms of sickle cell disease could potentially be added to the list of medical conditions in the future.
The main symptoms of sickle cell disease are fatigue and pain, and according to the state’s law, the commissioner of health may eventually add intractable pain to the list of qualifying medical conditions, making patients of sickle cell disease included.
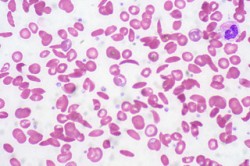
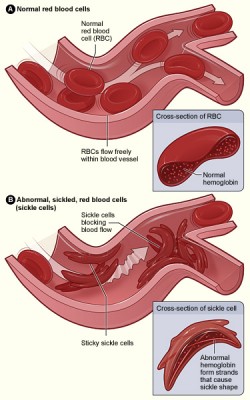
Sickle cell patients have crescent-shaped blood cells instead of healthy, disc-shaped ones. Sickle cells block blood flow and cause pain and organ damage, according to the National Heart, Lung and Blood Institute.
Former University student Brianna Wilson has sickle cell anemia that gives her bone and muscle pain.
“Some people describe it as nails poking you, but for me, it’s pressure in my veins and upper body,” she said.
Physicians usually prescribe opiates, like morphine, to treat the pain, but researchers and patients agree that there are better ways to treat the disease. Wilson said the drugs are addictive and usually don’t offer good results.
School of Dentistry professor and pain expert Donald Simone, who is also working on the research project, said opiates sometimes have “problematic” side effects, such as respiratory depression. And Gupta said patients sometimes receive incorrect dosages of the drugs because their exact amount of pain is unknown.
Developing a means to measure the severe pain could be useful for doctors while making prescriptions, said biomedical engineering professor Bin He, another researcher who is involved in the project.
Medical marijuana is promising for sickle cell patients because it has a pain-relieving effect without as many severe side effects as morphine, Simone said.
The National Institutes of Health awarded the researchers $9.5 million in January to pursue studies on mice and patients. With that money, the research is expanding to California to test the effects of vaporized cannabis on 35 sickle cell disease patients beginning in July.
So far, the researchers’ study has found that mice with sickle cell disease are more sensitive to pain, especially when experiencing pressure, heat or cold, Simone said. By examining how neurons in the peripheral nerves and the spinal cord become overactive, the researchers are able to identify new ways to reduce pain, he said.
University of California-San Francisco professor Donald Abrams, who will lead the clinical trials in partnership with the Minnesota researchers, said there were many “hoops to jump through” in going forward with the study, like gaining approval from numerous government agencies.
Currently, 22 states and the District of Columbia allow medical marijuana programs, all varying in levels of strictness.
Minnesota’s law is among the nation’s strictest, and it prohibits patients from smoking or growing their own marijuana plants. The law mandates that two manufacturers operate four distribution centers each and that medical marijuana identification cards be available beginning July 2015 through a state-monitored registry.
“I can see [medical marijuana] helping,” Wilson said. “It’s chronic pain, so it should help, especially if it’s relaxing the muscles and things like that.””
http://www.mndaily.com/news/campus/2014/06/10/medical-marijuana-could-treat-pain-caused-sickle-cell-disease
“Medical Marijuana Policies Complicate Research Treating Chronic Sickle Cell Pain. A study by University of Minnesota researchers that was testing the effects of medical marijuana in treating chronic pain experienced by sickle cell patients has been forced out of the state due to a combination of restrictive state and federal policies stalling the project.” http://www.huffingtonpost.com/2014/06/11/minnesota-medical-marijuana_n_5485383.html



1942-7611/asset/olalertbanner.jpg?v=1&s=4b27d6a6bed6b58a9935efe70e4f95efc39146bd)
