
 “Medical marijuana (MM) use is common among cancer patients, but relatively little is known about the usage patterns and efficacy of MM used by gynecologic cancer patients.
“Medical marijuana (MM) use is common among cancer patients, but relatively little is known about the usage patterns and efficacy of MM used by gynecologic cancer patients.
Methods: Demographic and clinical data were collected for gynecologic cancer patients prescribed MM between May 2016 and February 2019. The electronic medical record was used to query formulation prescribed, usage patterns, length of use, symptom relief, and side effect profile. Descriptive statistics were calculated.
Results: Of 45 gynecologic cancer patients prescribed MM, 89% were receiving chemotherapy; 56% were undergoing primary treatment. MM was used for a median of 5.2 months (range 0.6-25.4). Over 70% of patients reported improvement in nausea/vomiting, compared to 36% of patients using MM for pain relief (p = 0.02). Of 41 patients with follow-up information, 71% found MM improved at least one symptom.
Conclusions: Among a small sample of gynecologic cancer patients prescribed MM for symptom management, self-reported follow-up indicated symptom relief for the majority of patients and minimal therapy-related side effects. This data can prove useful for counseling gynecologic cancer patients on the efficacy and side effects of MM.”
“Among a small cohort of gynecologic cancer patients prescribed MM for symptom management, the majority reported improvement in at least one disease or treatment-related symptom and reported minimal side effects. Further larger prospective studies are needed to investigate specific formulations and indications in this patient population, but our data indicate that it is a safe and useful adjunct for symptom management among a diverse cohort of women with gynecologic cancer.”
https://www.sciencedirect.com/science/article/pii/S2352578921001247?via%3Dihub
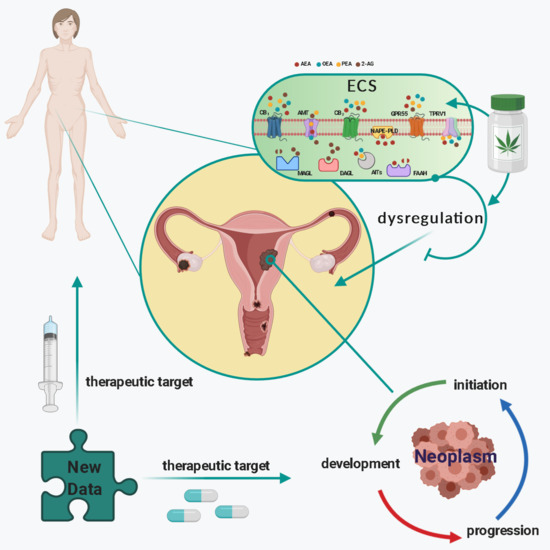
 “Cannabis has long been used for healing and recreation in several regions of the world. Over 400 bioactive constituents, including more than 100 phytocannabinoids, have been isolated from this plant. The non-psychoactive cannabidiol (CBD) and the psychoactive Δ9-tetrahydrocannabinol (Δ9-THC) are the major and widely studied constituents from this plant.
“Cannabis has long been used for healing and recreation in several regions of the world. Over 400 bioactive constituents, including more than 100 phytocannabinoids, have been isolated from this plant. The non-psychoactive cannabidiol (CBD) and the psychoactive Δ9-tetrahydrocannabinol (Δ9-THC) are the major and widely studied constituents from this plant. “Research within a gynecologic oncology population has lagged behind the uptake in use of medical cannabis for symptom control. This study seeks to evaluate patient experience with prescribed medical cannabis obtained through licensed dispensaries in women with gynecologic malignancies.
“Research within a gynecologic oncology population has lagged behind the uptake in use of medical cannabis for symptom control. This study seeks to evaluate patient experience with prescribed medical cannabis obtained through licensed dispensaries in women with gynecologic malignancies. “Providers need to be better equipped to discuss medical cannabis with patients even if they are not willing to prescribe it. The oncology community would be well served to ensure that providers are aware of existing cannabis research and are able to incorporate it into their communications with patients instead of leaving patients to figure out medical cannabis on their own.”
“Providers need to be better equipped to discuss medical cannabis with patients even if they are not willing to prescribe it. The oncology community would be well served to ensure that providers are aware of existing cannabis research and are able to incorporate it into their communications with patients instead of leaving patients to figure out medical cannabis on their own.”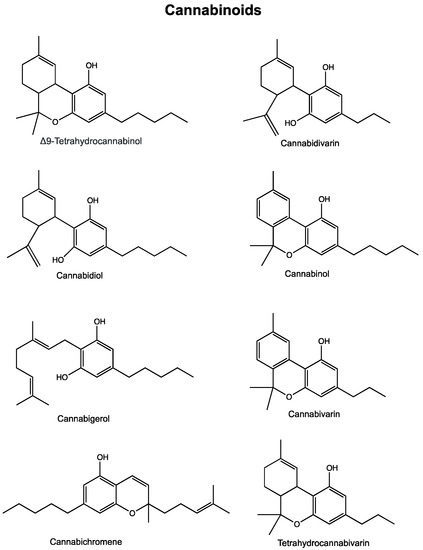
 “Phytocannabinoids are unique terpenophenolic compounds predominantly produced in the glandular trichomes of the cannabis plant (Cannabis sativa L.). The delta-9- tetrahydrocannabinol (THC) is the main active constituent responsible for the plant’s psychoactive effect and, together with the non- psychoactive cannabidiol (CBD), the most investigated naturally occurring cannabinoid.
“Phytocannabinoids are unique terpenophenolic compounds predominantly produced in the glandular trichomes of the cannabis plant (Cannabis sativa L.). The delta-9- tetrahydrocannabinol (THC) is the main active constituent responsible for the plant’s psychoactive effect and, together with the non- psychoactive cannabidiol (CBD), the most investigated naturally occurring cannabinoid.