“INTRODUCTION
: The increased incidence of Glioblastoma Multiforme, the most aggressive and most common primary brain tumour, is evident worldwide. Survival rates are reaching only 15 months due to its high recurrence and resistance to current combination therapies including oncotomy, radiotherapy and chemotherapy. Light has been shed in the recent years on the anticancer properties of cannabinoids from Cannabis sativa.
OBJECTIVE
: To determine whether cannabinoids alone or in combination with radiotherapy and/or chemotherapy inhibit tumour progression, induce cancer cell death, inhibit metastasis and invasiveness and the mechanisms that underlie these actions.
METHOD
: PubMed and Web of Science were used for a systemic search to find studies on the anticancer effects of natural cannabinoids on glioma cancer cells in vitro and/or in vivo.
RESULTS
: A total of 302 papers were identified, of which 14 studies were found to fit the inclusion criteria. 5 studies were conducted in vitro, 2 in vivo and 7 were both in vivo and in vitro. 3 studies examined the efficacy of CBD, THC and TMZ, 1 study examined CBD and radiation, 2 studies examined efficacy of THC only and 3 studies examined the efficacy of CBD only. 1 study examined the efficacy of CBD, THC and radiotherapy, 2 studies examined the combination of CBD and THC and 2 more studies examined the efficacy of CBD and TMZ.
CONCLUSION
: The evidence in this systematic review leads to the conclusion that cannabinoids possess anticancer potencies against glioma cells, however this effect varies with the combinations and dosages used. Studies so far were conducted on cells in culture and on mice as well as a small number of studies that were conducted on humans. Hence in order to have more accurate results, higher quality studies mainly including human clinical trials with larger sample sizes are necessitated urgently for GBM treatment.”
 “Cannabidiol (CBD) has been shown to slow cancer cell growth and is toxic to human glioblastoma cell lines. Thus, CBD could be an effective therapeutic for glioblastoma.
“Cannabidiol (CBD) has been shown to slow cancer cell growth and is toxic to human glioblastoma cell lines. Thus, CBD could be an effective therapeutic for glioblastoma.
 “Preclinical data suggest some cannabinoids may exert antitumour effects against glioblastoma (GBM). Safety and preliminary efficacy of nabiximols oromucosal cannabinoid spray plus dose-intense temozolomide (DIT) was evaluated in patients with first recurrence of GBM.
“Preclinical data suggest some cannabinoids may exert antitumour effects against glioblastoma (GBM). Safety and preliminary efficacy of nabiximols oromucosal cannabinoid spray plus dose-intense temozolomide (DIT) was evaluated in patients with first recurrence of GBM.
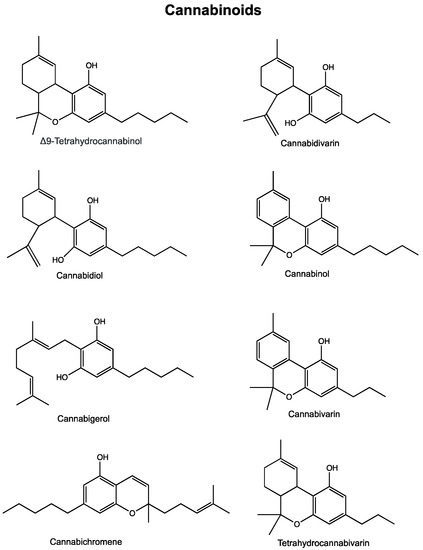
 “Cannabis has long been used for healing and recreation in several regions of the world. Over 400 bioactive constituents, including more than 100 phytocannabinoids, have been isolated from this plant. The non-psychoactive cannabidiol (CBD) and the psychoactive Δ9-tetrahydrocannabinol (Δ9-THC) are the major and widely studied constituents from this plant.
“Cannabis has long been used for healing and recreation in several regions of the world. Over 400 bioactive constituents, including more than 100 phytocannabinoids, have been isolated from this plant. The non-psychoactive cannabidiol (CBD) and the psychoactive Δ9-tetrahydrocannabinol (Δ9-THC) are the major and widely studied constituents from this plant. “Providers need to be better equipped to discuss medical cannabis with patients even if they are not willing to prescribe it. The oncology community would be well served to ensure that providers are aware of existing cannabis research and are able to incorporate it into their communications with patients instead of leaving patients to figure out medical cannabis on their own.”
“Providers need to be better equipped to discuss medical cannabis with patients even if they are not willing to prescribe it. The oncology community would be well served to ensure that providers are aware of existing cannabis research and are able to incorporate it into their communications with patients instead of leaving patients to figure out medical cannabis on their own.”