 “Fibromyalgia is a complex disease process that is as prevalent as it is poorly understood. Research into the pathophysiology is ongoing, and findings will likely assist in identifying new therapeutic options to augment those in existence today that are still insufficient for the care of a large population of patients.
“Fibromyalgia is a complex disease process that is as prevalent as it is poorly understood. Research into the pathophysiology is ongoing, and findings will likely assist in identifying new therapeutic options to augment those in existence today that are still insufficient for the care of a large population of patients.
Recent evidence describes the use of cannabinoids in the treatment of fibromyalgia.
This study provides a systematic, thorough review of the evidence alongside a review of the seminal data regarding the pathophysiology, diagnosis, and current treatment options.
Fibromyalgia is characterized by widespread chronic pain, fatigue, and depressive episodes without an organic diagnosis, which may be prevalent in up to 10% of the population and carries a significant cost in healthcare utilization, morbidity, a reduced quality of life, and productivity. It is frequently associated with psychiatric comorbidities. The diagnosis is clinical and usually prolonged, and diagnostic criteria continue to evolve. Some therapies have been previously described, including neuropathic medications, milnacipran, and antidepressants. Despite some level of efficacy, only physical exercise has strong evidence to support it.
Cannabis has been used historically to treat different pain conditions since ancient times.
Recent advances allowed for the isolation of the active substances in cannabis and the production of cannabinoid products that are nearly devoid of psychoactive influence and provide pain relief and alleviation of other symptoms. Many of these, as well as cannabis itself, are approved for use in chronic pain conditions.
Evidence supporting cannabis in chronic pain conditions is plentiful; however, in fibromyalgia, they are mostly limited. Only a handful of randomized trials exists, and their objectivity has been questioned. However, many retrospective trials and patient surveys suggest the significant alleviation of pain, improvement in sleep, and abatement of associated symptoms.
Evidence supporting the use of cannabis in chronic pain and specifically in fibromyalgia is being gathered as the use of cannabis increases with current global trends. While the current evidence is still limited, emerging data do suggest a positive effect of cannabis in fibromyalgia.
Cannabis use is not without risks, including psychiatric, cognitive, and developmental as well as the risks of addiction. As such, clinical judgment is warranted to weigh these risks and prescribe to patients who are more likely to benefit from this treatment. Further research is required to define appropriate patient selection and treatment regimens.”
https://pubmed.ncbi.nlm.nih.gov/33004171/
https://www.sciencedirect.com/science/article/pii/S1521689620300781?via%3Dihub

 “Objective: To determine the benefit of a tetrahydrocannabinol (THC)-rich cannabis oil on symptoms and quality of life of fibromyalgia patients.
“Objective: To determine the benefit of a tetrahydrocannabinol (THC)-rich cannabis oil on symptoms and quality of life of fibromyalgia patients. “The prevalence of cancer pain will continue to rise as pain is common among the survivorship and general cancer population. As interest in cannabis and cannabinoids for medicinal use including pain management continues to rise, there is growing need to update and review the current state of evidence for their use. The literature was searched for articles in English with key words cannabis, cannabinoids, and cancer pain. The sources of articles were PubMed, Embase, and open Google search.
“The prevalence of cancer pain will continue to rise as pain is common among the survivorship and general cancer population. As interest in cannabis and cannabinoids for medicinal use including pain management continues to rise, there is growing need to update and review the current state of evidence for their use. The literature was searched for articles in English with key words cannabis, cannabinoids, and cancer pain. The sources of articles were PubMed, Embase, and open Google search. “Although studied in a few randomized controlled trials (RCTs), the efficacy of medical cannabis (MC) for chronic pain remains controversial. Using an alternative approach, this multicenter, questionnaire-based prospective cohort was aimed to assess the long-term effects of MC on chronic pain of various etiologies and to identify predictors for MC treatment success.
“Although studied in a few randomized controlled trials (RCTs), the efficacy of medical cannabis (MC) for chronic pain remains controversial. Using an alternative approach, this multicenter, questionnaire-based prospective cohort was aimed to assess the long-term effects of MC on chronic pain of various etiologies and to identify predictors for MC treatment success.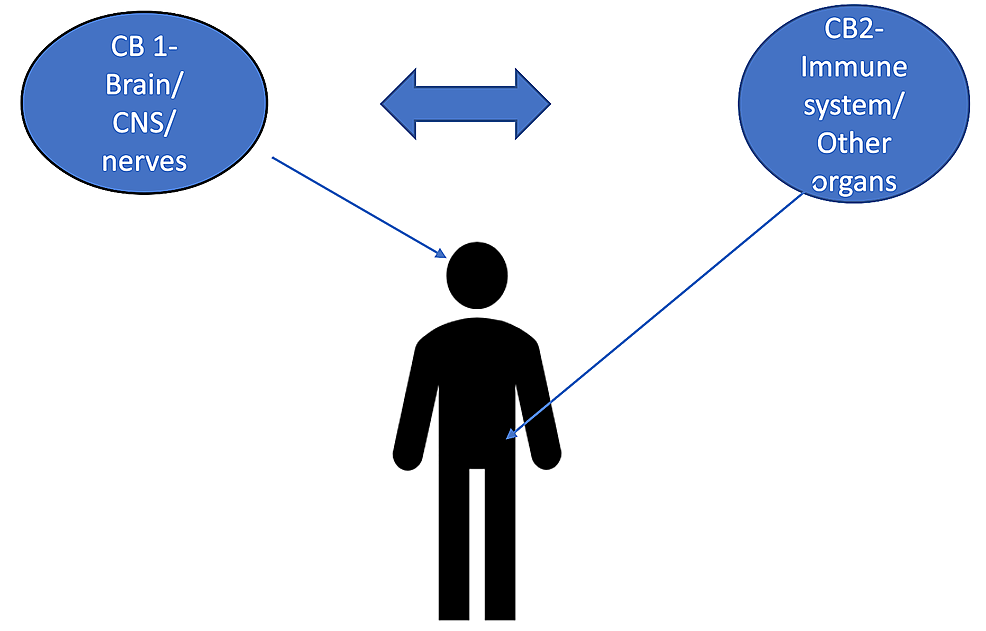 “The burden of chronic pain has affected many individuals leading to distress and discomfort, alongside numerous side effects with conventional therapeutic approaches.
“The burden of chronic pain has affected many individuals leading to distress and discomfort, alongside numerous side effects with conventional therapeutic approaches. “Cannabinoids help in pain treatment through their action on CB1 and CB2 receptors.
“Cannabinoids help in pain treatment through their action on CB1 and CB2 receptors. “Rett syndrome (RTT) is a rare neurologic disorder, characterized by severe behavioural and physiological symptoms. RTT is caused by mutations in the MECP2 gene in about 95% of cases and to date no cure is available.
“Rett syndrome (RTT) is a rare neurologic disorder, characterized by severe behavioural and physiological symptoms. RTT is caused by mutations in the MECP2 gene in about 95% of cases and to date no cure is available. “Cannabis exposure is becoming more common in older age but little is known about how it is associated with brain health in this population.
“Cannabis exposure is becoming more common in older age but little is known about how it is associated with brain health in this population.