“Diabetes is a chronic disease associated with a high number of complications such as peripheral neuropathy, which causes sensorial disturbances and may lead to the development of diabetic neuropathic pain (DNP). The current treatment for DNP is just palliative and the drugs may cause severe adverse effects, leading to discontinuation of treatment. Thus, new therapeutic targets need to be urgently investigated.
“Diabetes is a chronic disease associated with a high number of complications such as peripheral neuropathy, which causes sensorial disturbances and may lead to the development of diabetic neuropathic pain (DNP). The current treatment for DNP is just palliative and the drugs may cause severe adverse effects, leading to discontinuation of treatment. Thus, new therapeutic targets need to be urgently investigated.
Studies have shown that cannabinoids have promising effects in the treatment of several pathological conditions, including chronic pain.
Thus, we aimed to investigate the acute effect of the intrathecal injection of CB1 or CB2 cannabinoid receptor agonists N-(2-chloroethyl)-5Z, 8Z, 11Z, 14Z-eicosatetraenamide (ACEA) or JWH 133, respectively (10, 30 or 100 μg/rat) on the mechanical allodynia associated with experimental diabetes induced by streptozotocin (60 mg/kg; intraperitoneal) in rats.
Cannabinoid receptor antagonists CB1 AM251 or CB2 AM630 (1 mg/kg) were given before treatment with respective agonists to confirm the involvement of cannabinoid CB1 or CB2 receptors. Rats with diabetes exhibited a significant reduction on the paw mechanical threshold 2 weeks after diabetes induction, having the maximum effect observed 4 weeks after the streptozotocin injection. This mechanical allodynia was significantly improved by intrathecal treatment with ACEA or JWH 133 (only at the higher dose of 100 μg). Pre-treatment with AM251 or AM630 significantly reverted the anti-allodynic effect of the ACEA or JWH 133, respectively.
Considering the clinical challenge that the treatment of DPN represents, this study showed for the first time, that the intrathecal cannabinoid receptors agonists may represent an alternative for the treatment of DNP.”
 “The contribution of substance use disorders to the burden of severe maternal morbidity in the United States is poorly understood. The objective was to estimate the independent association between substance use disorders during pregnancy and risk of severe maternal morbidity.
“The contribution of substance use disorders to the burden of severe maternal morbidity in the United States is poorly understood. The objective was to estimate the independent association between substance use disorders during pregnancy and risk of severe maternal morbidity. “Posttraumatic stress disorder (PTSD) may stem from the formation of aberrant and enduring aversive memories. Some PTSD patients have recreationally used Cannabis, probably aiming at relieving their symptomatology.
“Posttraumatic stress disorder (PTSD) may stem from the formation of aberrant and enduring aversive memories. Some PTSD patients have recreationally used Cannabis, probably aiming at relieving their symptomatology.
 “Few studies to date have measured the real-time effects of consumption of common and commercially available Cannabis products for the treatment of headache and migraine under naturalistic conditions. This study examines, for the first time, the effectiveness of using dried Cannabis flower, the most widely used type of Cannabis product in the United States, in actual time for treatment of headache- and migraine-related pain and the associations between different product characteristics and changes in symptom intensity following Cannabis use.
“Few studies to date have measured the real-time effects of consumption of common and commercially available Cannabis products for the treatment of headache and migraine under naturalistic conditions. This study examines, for the first time, the effectiveness of using dried Cannabis flower, the most widely used type of Cannabis product in the United States, in actual time for treatment of headache- and migraine-related pain and the associations between different product characteristics and changes in symptom intensity following Cannabis use. “Chronic ethanol abuse can lead to harmful consequences for the heart, resulting in systolic dysfunction, variability in the heart rate, arrhythmia, and cardiac remodelling. However, the precise molecular mechanism responsible for ethanol-induced cardiomyopathy is poorly understood. In this regard, the present study aimed to describe the RIP1/RIP3/MLKL-mediated necroptotic cell death that may be involved in ethanol-induced cardiomyopathy and characterize CBR-mediated effects on the signalling pathway and myocardial injury.
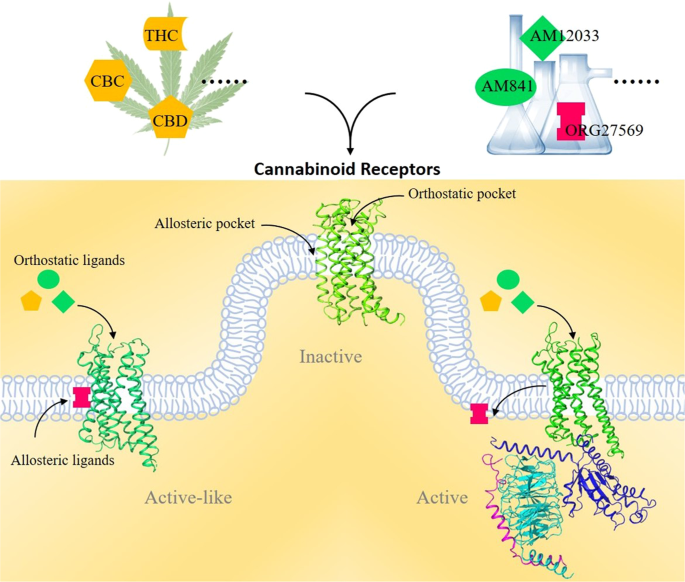
“Chronic ethanol abuse can lead to harmful consequences for the heart, resulting in systolic dysfunction, variability in the heart rate, arrhythmia, and cardiac remodelling. However, the precise molecular mechanism responsible for ethanol-induced cardiomyopathy is poorly understood. In this regard, the present study aimed to describe the RIP1/RIP3/MLKL-mediated necroptotic cell death that may be involved in ethanol-induced cardiomyopathy and characterize CBR-mediated effects on the signalling pathway and myocardial injury. “Cannabinoids (CBs), analgesic drugs used for thousands of years, were first found in Cannabis sativa, and the multiple CBs used medicinally, such as tetrahydrocannabinol (THC), cannabidiol (CBD) and dozens more, have complex structures. In addition to their production by plants, CBs are naturally present in the nerves and immune systems of humans and animals.
“Cannabinoids (CBs), analgesic drugs used for thousands of years, were first found in Cannabis sativa, and the multiple CBs used medicinally, such as tetrahydrocannabinol (THC), cannabidiol (CBD) and dozens more, have complex structures. In addition to their production by plants, CBs are naturally present in the nerves and immune systems of humans and animals.