
 “Medical cannabis and individual cannabinoids, such as tetrahydrocannabinol (THC) and cannabidiol (CBD), are receiving growing attention in both the media and the scientific literature. The Cannabis plant, however, produces over 100 different cannabinoids, and cannabigerol (CBG) serves as the precursor molecule for the most abundant phytocannabinoids.
“Medical cannabis and individual cannabinoids, such as tetrahydrocannabinol (THC) and cannabidiol (CBD), are receiving growing attention in both the media and the scientific literature. The Cannabis plant, however, produces over 100 different cannabinoids, and cannabigerol (CBG) serves as the precursor molecule for the most abundant phytocannabinoids.
CBG exhibits affinity and activity characteristics between THC and CBD at the cannabinoid receptors, but appears to be unique in its interactions with alpha-2 adrenoceptors and 5-HT1A Studies indicate that CBG may have therapeutic potential in treating neurological disorders (e.g., Huntington’s Disease, Parkinson’s Disease, and multiple sclerosis), inflammatory bowel disease, as well as having antibacterial activity.
There is growing interest in the commercial use of this unregulated phytocannabinoid. This review focuses on the unique pharmacology of CBG, our current knowledge of its possible therapeutic utility, and its potential toxicological hazards.
Significance Statement Cannabigerol (CBG) is currently being marketed as a dietary supplement and, as with cannabidiol (CBD) before, many claims are being made about its benefits. Unlike CBD, however, little research has been performed on this unregulated molecule, and much of what is known warrants further investigation to identify potential areas of therapeutic uses and hazards.”
https://pubmed.ncbi.nlm.nih.gov/33168643/
https://jpet.aspetjournals.org/content/early/2020/11/09/jpet.120.000340
 “The aberrant accumulation of disease-specific protein aggregates accompanying cognitive decline is a pathological hallmark of age-associated neurological disorders, also termed as proteinopathies, including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, amyotrophic lateral sclerosis and multiple sclerosis.
“The aberrant accumulation of disease-specific protein aggregates accompanying cognitive decline is a pathological hallmark of age-associated neurological disorders, also termed as proteinopathies, including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, amyotrophic lateral sclerosis and multiple sclerosis.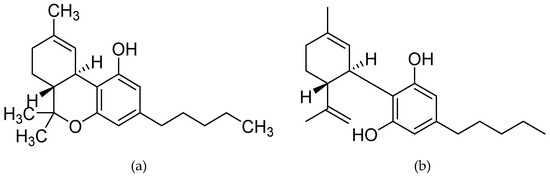
 “Δ9 -Tetrahydrocannabinol (THC), the main bioactive compound found in the plant Cannabis sativa, exerts its effects by activating cannabinoid receptors present in many neural cells.
“Δ9 -Tetrahydrocannabinol (THC), the main bioactive compound found in the plant Cannabis sativa, exerts its effects by activating cannabinoid receptors present in many neural cells. “Objectives
“Objectives
 “Objectives: To investigate the action of cannabinoids on spasticity and pain in secondary progressive multiple sclerosis, by means of neurophysiological indexes.
“Objectives: To investigate the action of cannabinoids on spasticity and pain in secondary progressive multiple sclerosis, by means of neurophysiological indexes. “Painful tonic spasm (PTS) is a common yet debilitating symptom in patients with neuromyelitis optica spectrum disorder (NMOSD), especially those with longitudinally extensive transverse myelitis. Although carbamazepine is an effective treatment, it poses the risk of severe adverse reactions, such as Steven-Johnson syndrome (SJS).
“Painful tonic spasm (PTS) is a common yet debilitating symptom in patients with neuromyelitis optica spectrum disorder (NMOSD), especially those with longitudinally extensive transverse myelitis. Although carbamazepine is an effective treatment, it poses the risk of severe adverse reactions, such as Steven-Johnson syndrome (SJS). “Cannabidiol (
“Cannabidiol (